How Does Chiropractic Help with Headaches?
Since 9 out of 10 Americans suffer from some form of headache, we tend to think of them as just a nuisance that can be relieved by taking a painkiller or a nap. Those solutions sometimes lighten the pain momentarily, but recurring headaches are a symptom that something else is wrong, and finding the root cause of your headaches is imperative to putting an end to them.
Fortunately, there’s a proven alternative. According to a new study, chiropractic treatment can provide “immediate relief” for many headache patients.
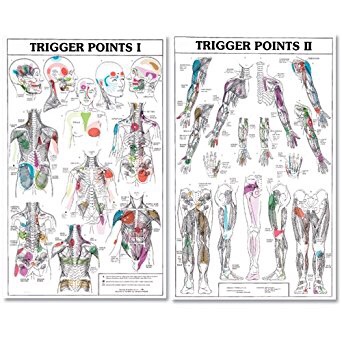
The majority of primary headaches, including tension headaches and migraines, are frequently associated with muscle tension or joint restrictions in the neck. These problems occur more often than ever before because nowadays we’re sitting in front of the computer for hours at a time or looking down at a phone to surf the web or text.
Chiropractors work to remove the triggers of these painful problems like stiffness, tightness, inflammation, and nerve irritation in the cervical spine. In addition to performing gentle spinal manipulation and soft tissue release, your chiropractor can also provide nutritional advice to help you avoid common migraine triggers found in your diet. Many patients also benefit from chiropractic advice on posture, relaxation techniques, and exercises to help prevent future problems.
So, if you or someone you know suffers from headache, call our office today. And check out this short video for more information about relief for neck-related headaches.