What is health?
Ergonomics is the science of adjusting your workstation to minimize strain in the following ways:
✓ Maintain proper body position and alignment while sitting at your desk – Hips, knees and elbows at 90 degrees, shoulders relaxed, feet flat on floor or footrest.
✓ Wrists should not be bent while at the keyboard. Forearms and wrists should not be leaning on a hard edge.
✓ Use audio equipment that keeps you from bending your neck (i.e., Bluetooth, speakerphones, headsets).
✓ Monitors should be visible without leaning or straining and the top line of type should be 15 degrees below eye level.
✓ Use a lumber roll for lower back support.
✓ Avoid sitting on anything that would create an imbalance or uneven pressure (like your wallet).
✓ Take a 10-second break every 20 minutes: Micro activities include: standing, walking, or moving your head in a “plus sign” fashion.
✓ Periodically, perform the “Brugger relief position” (See video below) -Position your body at the chair’s edge, feet pointed outward. Weight should be on your legs and your abdomen should be relaxed. Tilt your pelvis forward, lift your sternum, arch your back, drop your arms, and roll out your palms while squeezing your shoulders together. Take a few deep cleansing breaths.

The masseter is the main muscle that moves your jaw. It originates on the zygomatic arch and maxilla, and inserts on the coronoid process and Ramus of the mandible. It’s actions are to elevate the mandible and close the jaw. The deep fibres of this muscle also retrude the mandible. This muscle commonly harbours trigger points as a result of teeth grinding. Trigger points in this muscle are often also associated with tmj dysfunction. Trigger points in the upper part of this muscle will refer pain to the upper molars and maxilla often felt as sinusitis. Trigger points in the lower portion of this muscle refer to the lower molars and temple. All trigger points can cause tooth sensitivity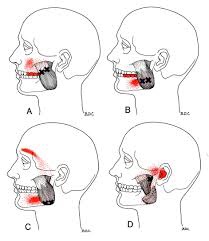
Whiplash, or “Whiplash Associated Disorders” or WAD, is the result of a sudden “crack the whip” of the head on the neck due to a slip and fall, sports injury, a violent act, or most commonly, a motor vehicle collision (MVC), particularly a rear-end collision. In describing “what can I expect” after a whiplash injury, one thing is for certain, there are many faces of whiplash, meaning the degree of injury can range from none to catastrophic depending on many factors, some of which are difficult or impossible to identify or calculate. Let’s take a closer look!
Even though the good news is that most people injured in a car crash get better, 10% do not and go on to have chronic pain, of which about half have significant difficulty working and/or doing desired everyday activities. There is a “great debate” as to the way experts describe “chronic whiplash syndrome” (CWS) as well as how these cases should be managed. Some feel there is something PHYSICALLY wrong in the CWS patient, especially if severe neck or head pain persists for more than one year. There is some proof of this as Dr. Nikolai Bogduk from the University of Newcastle in Australia and colleagues have used selective nerve blocks to anesthetize specific joints in the neck to determine exactly where the pain is generated. The patient then has the option to have that nerve cauterized or burned and pain relief can be significant in many cases. Dr. Bogduk and his group admit that these CWS patients have more psychological symptoms, but they feel this is the result of pain, not the CAUSE.
On the other hand, experts such as Dr. Henry Berry from the University of Toronto report the EXACT OPPOSITE. He argues that it’s not JUST the physical injury that has to be dealt with but also the person’s “state of mind.” Dr. Berry states that when stepping back and looking at all the complaints or symptoms from a distance, “…you see these symptoms can be caused by life stress, the illness ‘role’ as a way of adjusting to life, psychiatric disorders, or even [made up by the patient].” Berry contends that it’s important to tell the patient their pain will go away soon, advises NO MORE THAN two weeks of physical therapy, and sends people back to work ASAP.
Oregon Health Sciences University School of Medicine’s Dr. Michael D. Freeman, whose expertise lay in epidemiology and forensic science, disagrees with Dr. Berry stating that the scientific literature clearly supports the physical injury concept and states, “…the idea that it is a psychological disturbance is a myth that has been perpetuated with absolutely no scientific basis at all.” Dr. Freeman states that 45% of people with chronic neck pain were injured in a motor vehicle crash (which includes three million of the six million of those injured in car crashes every year in the United States).
Here’s the “take home” to consider: 1) CWS occurs in about 10% of rear-end collisions; 2) Some doctors feel the pain is physically generated from specific nerves inside the neck joints; 3) Others argue it’s a combination of psychological factors and care should focus on preventing sufferers from becoming chronic patients.
Many studies report that chiropractic offers fast, cost-effective benefits for whiplash-injured patients with faster return to work times and higher levels of patient satisfaction.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honored to render our services.
To avoid extra stress on your spine while standing:
✓ Avoid high-heeled shoes or boots
✓ Use a footrest measuring 10% of your height
✓ To decrease stress on your back and feet consider leaning on a tall chair.
✓ If excessive standing can’t be avoided, consider shock-absorbent shoes or an anti-fatigue mat.
✓ When transitioning from a sitting workstation to a standing desk, begin gradually by standing 20 minutes per hour and not necessarily in a continuous period. Add an extra 10 minutes per hour each day as long as there is no prolonged stiffness or discomfort.
Headaches are REALLY common! In fact, two out of three children will have a headache by the time they are fifteen years old, and more than 90% of adults will experience a headache at some point in their life. It appears safe to say that almost ALL of us will have firsthand knowledge of what a headache is like sooner or later!
Certain types of headaches run in families (due to genetics), and headaches can occur during different stages of life. Some have a consistent pattern, while others do not. To make this even more complicated, it’s not uncommon to have more than one type of headache at the same time!
Headaches can vary in frequency and intensity, as some people can have several headaches in one day that come and go, while others have multiple headaches per month or maybe only one or two a year. Headaches may be continuous and last for days or weeks and may or may not fluctuate in intensity.
For some, lying down in a dark, quiet room is a must. For others, life can continue on like normal. Headaches are a major reason for missed work or school days as well as for doctor visits. The “cost” of headaches is enormous—running into the billions of dollars per year in the United States (US) in both direct costs and productivity losses. Indirect costs such as the potential future costs in children with headaches who miss school and the associated interference with their academic progress are much more difficult to calculate.
There are MANY types of headaches, which are classified into types. With each type, there is a different cause or group of causes. For example, migraine headaches, which affect about 12% of the US population (both children and adults), are vascular in nature—where the blood vessels dilate or enlarge and irritate nerve-sensitive tissues inside the head. This usually results in throbbing, pulsating pain often on one side of the head and can include nausea and/or vomiting. Some migraine sufferers have an “aura” such as a flashing or bright light that occurs within 10-15 minutes prior to the onset while other migraine sufferers do not have an aura.
The tension-type headache is the most common type and as the name implies, is triggered by stress or some type of tension. The intensity ranges between mild and severe, usually on both sides of the head and often begin during adolescence and peak around age 30, affecting women slightly more than men. These can be episodic (come and go, ten to fifteen times a month, lasting 30 min. to several days) or chronic (more than fifteen times a month over a three-month period).
There are many other types of headaches that may be primary or secondary—when caused by an underlying illness or condition. The GOOD news is chiropractic care is often extremely helpful in managing headaches of all varieties and should be included in the healthcare team when management requires a multidisciplinary treatment approach.
Most of know someone who has been affected by headaches. If they are looking for help and information please feel free to contact us at 204-586-8424 or at info@aberdeenchiropractic.com.
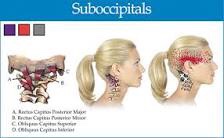
The suboccipitals are a group or four muscles that attach to the transverse and spinous process of C1 and C2 and the occipital bone.
These muscles provide extension side bending and rotation movements between the occiput and C1 and C2. These muscles are often overloaded due to postural strain. A classic example being sitting in front of a computer all day.
When these muscles are overloaded trigger points can develop. Pain and symptoms of trigger points in the suboccipitals include head pain that penetrates into the skull but is difficult to localize.
Patients are likely to describe the pain as “all over” including the occiput, eye and forehead, but without any clarity. Trigger points in these muscles are often associated with tension head aches
.
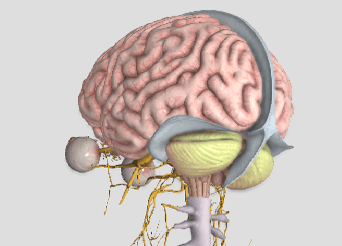
In a 2010 study, researchers examined MRIs taken from 1,200 patients (600 whiplash and 600 non-whiplash neck pain patients) and noted that those who had sustained whiplash were more likely to have a brain injury than non-whiplash neck pain patients.
The specific type of brain injury found is a form of herniation called Chiari malformation, where the bottom part of the brain (the cerebellum) drops through the opening in the base of the skull called the foramen magnum. Their findings showed an alarming 23% of the whiplash cases studied had this anatomical abnormality.
Dr. Michael Freeman, Dr. Ezriel Kormel, and colleagues collaborated in this effort and evaluated the patients using MRI in both recumbent (laying down) AND upright positions. Interestingly, they found 5.7% and 5.3% of those in the non-whiplash neck pain group and 9.8% and 23.3% in the whiplash group had the Chiari malformation using the recumbent vs. upright MRI positions, respectfully.
Dr. Kormel stated, “This condition can be quite painful and endanger the patient’s health, with symptoms that may include headaches, neck pain, upper extremity numbness and tingling, and weakness. In a few cases, there can also be lower extremity weakness and brain dysfunction.” In a radio interview, he added the advice that ANYONE suffering from whiplash should see a healthcare provider immediately.
This study is important for a number of reasons. First, it revealed that there is often a more serious injury when whiplash occurs than what is initially found. Second, psychological findings like depression, anxiety, and difficulty coping with the decreased ability or inability to be productive at home or work may suggest the presence of an anatomical injury which simply has not yet been found. Third, MRI is frequently ONLY performed in a laying down position. This study didn’t find much difference between laying vs. weight-bearing MRI positions in the non-whiplash neck pain patients but not so in the whiplash neck pain group! In this group, the ability for MRI to detect Chiari malformation/brain injury more than doubled using weight-bearing MRI.
Expanding the last point, since one out of five whiplash patients had a brain injury that is more likely to be detected using a non-traditional upright MRI position, a “new” standard” for the use of MRI in the evaluation of the whiplash patient should be considered. This is especially important in those cases that are non-responsive to quality care or if their doctor had only ordered a recumbent MRI previously.
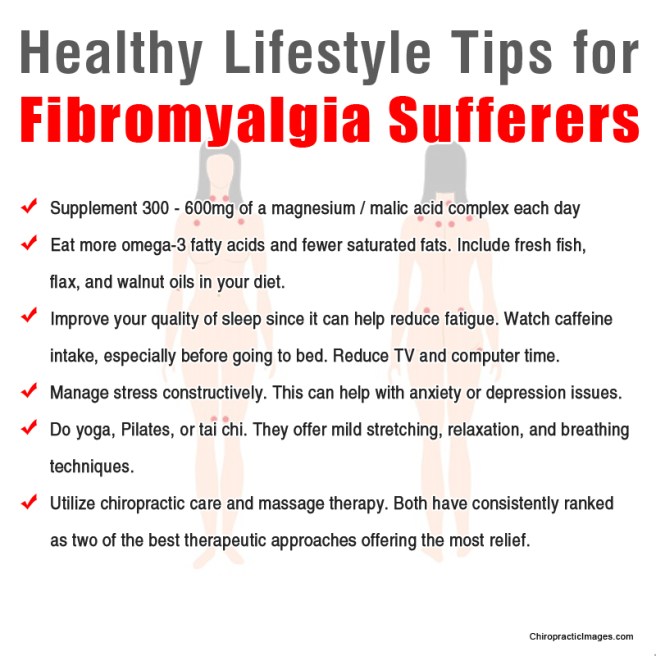
Are there differences in lifestyle between people with vs. without fibromyalgia (FM)?
A recent study found women with FM found spend more time engaged in sedentary behaviors and less time in physical activity. In the study, researchers followed 413 female patients with FM and 188 age-matched healthy female controls. Researchers used three different approaches to access physical activity: a triaxial accelerometer to examine sedentary time, time spent in physical activity, and step counts.
They discovered those who suffered from FM spent an average of 39 more minutes per day in sedentary activity and 21 fewer minutes per day in light physical activity, 17 fewer minutes per day in moderate physical activity, and 19 fewer minutes per day in moderate-to-vigorous physical activity. In addition, those with FM took a mean of 1,881 fewer steps that those without FM.
Now, this isn’t really a surprise given the fact that people with FM are in pain and more likely to have difficulties sleeping and tolerating prolonged activities. After comparing the sufferers to the non-sufferers, the researchers found only 21% of FM patients vs. 46% of non-FM controls achieved the recommended 150 minutes/week (a little over 20 min. / day) of “moderate-to-vigorous” physical activity. They also found that only 16% vs. 45%, respectively, walked the recommended ≥10,000 steps per day.
One of the BEST forms of exercise for most people is walking. A walking program should be a staple exercise. It’s important to note that this should be GRADUALLY introduced so as to avoid an overuse injury—strain or sprain of the muscles and joints. This gradual introduction into activity is ESPECIALLY important for the FM sufferer as overuse injuries can make them afraid to do something that can REALLY help when done correctly!