The Levator scapula is a muscle in your neck that originates on the transverse processes of C1-C4 and inserts on the superior part of the medial border of the scapula. The primary actions of this muscle are to elevate the scapula and rotate the glenoid fossa downward. It also rotates the neck to the same side and assists in extension. When this muscle is tight it restricts neck rotation resulting in the classic “stiff neck”. With a forward head position the Levator is often stretched and over worked. To help combat this you must get the head back by releasing the anterior chest and neck muscles. Trigger points in this muscle refer pain into the angle of the neck and down the shoulder blade.
Myofascial Pain
Hip Abductor Weakness

* The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance.
* Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity.
* There is no “typical” presentation for hip abductor weakness, but the problem must be considered in any patient with lower chain symptomatology, particularly those with hip tendinopathy, greater trochanteric pain syndrome, iliotibial band syndrome, patellofemoral pain syndrome, ACL injury, medial knee pain, and lower back pain.
*Hip abductor weakness is often accompanied by lower crossed syndrome – a larger pattern of biomechanical dysfunction involving weakness of the abdominal wall and hypertonicity in the hip flexors and paraspinal musculature. Evaluation should include a relatively global assessment of lumbopelvic muscle and joint function. Additionally, clinicians should assess for the presence of foot hyperpronation in patients with hip abductor weakness.
Referenced from:
ChiroUp.com “Hip Abductor Weakness Clinical Pearls
Trigger points in the masseter muscle

The masseter is the main muscle that moves your jaw. It originates on the zygomatic arch and maxilla, and inserts on the coronoid process and Ramus of the mandible. It’s actions are to elevate the mandible and close the jaw. The deep fibres of this muscle also retrude the mandible. This muscle commonly harbours trigger points as a result of teeth grinding. Trigger points in this muscle are often also associated with tmj dysfunction. Trigger points in the upper part of this muscle will refer pain to the upper molars and maxilla often felt as sinusitis. Trigger points in the lower portion of this muscle refer to the lower molars and temple. All trigger points can cause tooth sensitivity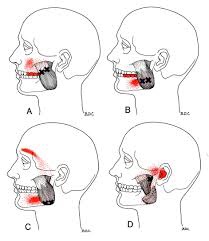
Trigger points in the suboccipitals.
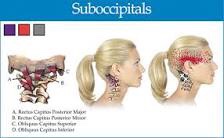
The suboccipitals are a group or four muscles that attach to the transverse and spinous process of C1 and C2 and the occipital bone.
These muscles provide extension side bending and rotation movements between the occiput and C1 and C2. These muscles are often overloaded due to postural strain. A classic example being sitting in front of a computer all day.
When these muscles are overloaded trigger points can develop. Pain and symptoms of trigger points in the suboccipitals include head pain that penetrates into the skull but is difficult to localize.
Patients are likely to describe the pain as “all over” including the occiput, eye and forehead, but without any clarity. Trigger points in these muscles are often associated with tension head aches
.
Our Exercise Of The Month: ITB Foam Roller
ITB – Foam Roller
- Lie on your side with your affected thigh over a foam roll.
- Lift your shoulders off of the floor with your arm and roll the fleshy part your mid & lower thigh back and forth over the foam roller.
- Avoid rolling over the bony point of your hip unless specifically directed.
- Perform this exercise for one minute twice per day or as directed.
Trigger points in the sternocleidomastoid muscle. By Bryan Cobb RMT.

The sternocleidomastoid muscle or “scm” is a strap like muscle located in the front of the neck. It originates on the manubrium of the sternum and the medial clavicle, and inserts on the mastoid process of the temporal bone( the lump or bone behind the ear). When working together the scm flexes the head and neck. The actions of one muscle working by itself is to rotate the face to the opposite side and lift it toward the ceiling.
Trigger points in this muscle usually form due to acute injury or to chronic postural stress. These trigger points can cause a wide variety of symptoms including pain felt in the cheek, temple, forehead, top of the head, and base of the skull. Trigger points in these muscles can also refer deep into the ear and cause postural dizziness.
Exercise Of The Month: Pike On A Ball
Pike on a Ball
Begin in a push-up position with your knees resting on an exercise ball. Maintain a neutral spine, and do not allow your back to arch down towards the floor. Roll the ball from your thighs to your ankles by bending your knees and bringing them towards your chest. Slowly return to the start position. Perform three sets of 10 repetitions daily or as directed.
Condition Of The Month: Pregnancy-Related Low Back Pain

Low back pain during pregnancy is quite common. In fact, between 50-75% of all pregnant women will experience low back pain. The pain is usually caused from rapid changes in weight, posture, gait and hormones.
The average woman gains between 20-40 pounds throughout pregnancy. This weight gain moves your center of gravity forward, causing your pelvis to tilt and your lower back to sway – placing excessive stress on the ligaments, discs, and joints of your spine.
Pregnancy-related low back pain typically starts between the fifth and seventh month of pregnancy, although a significant portion of women experience pain sooner. Symptoms often begin at the base of your spine and may radiate into your buttock or thigh. Discomfort is often aggravated by prolonged standing, sitting, coughing, or sneezing. Your symptoms may increase throughout the day, and some patients report nighttime pain that disturbs their sleep. The extremes of activity seem to contribute to pregnancy-related low back pain – with increased risk for both “sedentary” and “physically demanding” lifestyles. Patients who have suffered with back pain prior to pregnancy are more than twice as likely to re-develop back pain during pregnancy.
Be sure to tell your doctor if your symptoms include fever, chills, bleeding, spotting, unusual discharge, cramping, sudden onset pelvis pain, light-headedness, shortness of breath, chest pain, headache, calf pain or swelling, decreased fetal movement, or symptoms that radiate beyond your knee.
Unfortunately, pregnancy related low back pain occurs at a time when your medical treatment options are limited. Not surprisingly, over 90% of prenatal health care providers would recommend drug-free treatment, including the type of alternative therapy provided in this office. Studies have shown that chiropractic manipulation provides significant relief of pregnancy- related low back pain. Almost 75% of women undergoing chiropractic care report significant pain reduction with improved ability to function.
Most patients will also benefit from continuing aerobic exercise throughout pregnancy. The US Department of Health and Human Services advises that healthy pregnant women may begin or continue moderate intensity aerobic exercise for at least 150 minutes per week. Women should not begin “vigorous” exercise during pregnancy, but those who were preconditioned to vigorous exercise may continue. Be sure to check with your doctor prior to initiating or increasing any exercise program while you are pregnant.
Be sure to take frequent breaks from prolonged sitting or standing. You may find benefit by using a small footstool to alternate feet while standing. Sleeping with a pillow between the knees in a side lying posture may help you to rest more comfortably. You should wear shoes with good arch supports. In some cases, your chiropractor may recommend a sacroiliac belt or pelvic support belt to help relieve your pregnancy-related low back pain.
I love this video
There is a lot to be learnt from this video. Dr. Mike Evans does a great job of explaining why we need to KEEP MOVING during and after an episode of low back pain. Check it out!
PFPS Cont. You want details?

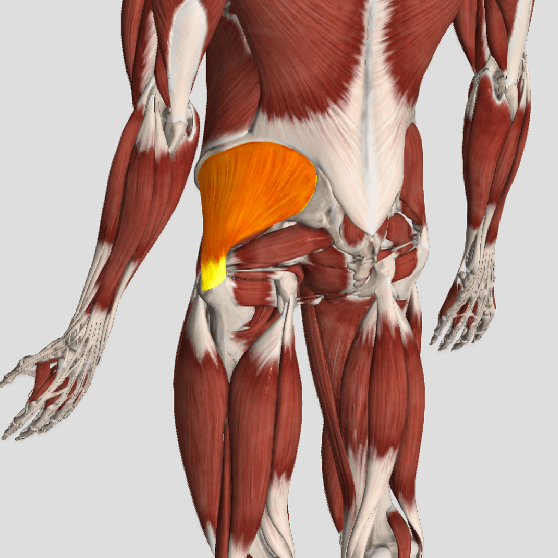
The muscles of the hip provide not only local stability, but also play an important role in spinal and lower extremity functional alignment. (1-4) While weakness in some hip muscles (hip extensors and knee extensors) is well tolerated, weakness or imbalance in others can have a profound effect on gait and biomechanical function throughout the lower half of the body. (5) Weakness of the hip abductors, particularly those that assist with external rotation, has the most significant impact on hip and lower extremity stability. (5,6)
The gluteus medius is the principal hip abductor. When the hip is flexed, the muscle also assists the six deep hip external rotators (piriformis, gemelli, obturators, and quadratus femoris). The gluteus medius originates on the ilium just inferior to the iliac crest and inserts on the lateral and superior aspects of the greater trochanter. While the principal declared action of the gluteus medius is hip abduction, clinicians will appreciate its more valuable contribution as a dynamic stabilizer of the hip and pelvis- particularly during single leg stance activities like walking, running, and squatting. The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance. The remainder comes predominantly from 2 muscles that insert onto the iliotibial band: the tensor fascia lata and upper gluteus maximus. Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity. (6)
Incompetent hip abductors and/or external rotators allows for excessive adduction and internal rotation of the thigh during single leg stance activities. This leads to a cascade of biomechanical problems, including pelvic drop, excessive hip adduction, excessive femoral internal rotation, valgus knee stress, and internal tibial rotation. (1,7-12)
