This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.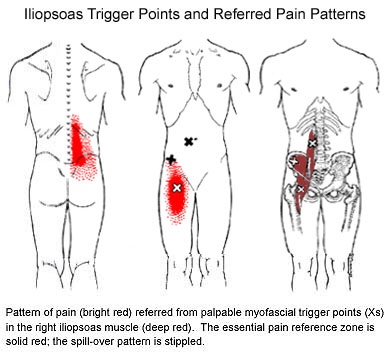
Myofascial Pain
My abductors are weak, what does that mean?
One very important job of your hip muscles is to maintain the alignment of your leg when you move. One of the primary hip muscles, the gluteus medius, plays an especially important stabilizing role when you walk, run, or squat. The gluteus medius attaches your thigh bone to the crest of your hip. When you lift your left leg, your right gluteus medius must contract in order to keep your body from tipping toward the left. And when you are standing on a bent leg, your gluteus medius prevents that knee from diving into a “knock knee” or “valgus” position. 
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
You should avoid activities that cause prolonged stretching of the hip abductors, like “hanging on one hip” while standing, sitting crossed legged, and sleeping in a side-lying position with your top knee flexed and touching the bed. Patients with fallen arches may benefit from arch supports or orthotics. Obesity causes more stress to the hip muscles, so overweight patients may benefit from a diet and exercise program. The most important treatment for hip abductor weakness is strength training. Hip strengthening is directly linked to symptom improvement. Moreover, people with stronger hip muscles are less likely to become injured in the first place. The exercises listed below are critical for your recovery.
Meet the Hip Cycle. You can thank me later.
1. Side lying with back and shoulders against a wall so you can’t roll back.
2. Bend your bottom leg and put the sole of your foot against the wall to be more stable.
3. Start position is with your foot directly in line with your hip. Do not let it get any lower than that. The highest point of your foot needs to be the bump on the outside of your ankle.
Do 5-10 reps of each of the following without rest between exercises twice a day. The goal is 20 reps each.
a. 6″ leg raises in abduction
b. Knee up to chest (90* knee and hip)
c. 12″ leg raises into abduction
d. Bicycling (knee up to chest, extend knee and sweep back to start with leg straight)
e. Clockwise circles
f. Counterclockwise circles
Good luck.
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 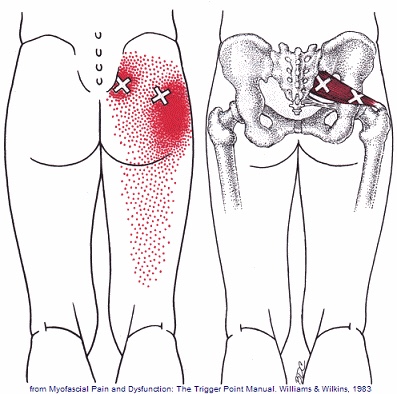
Piriformis Syndrome; a real bummer.
Piriformis syndrome results from compression of the sciatic nerve as it passes underneath a muscle in your buttock called the piriformis. Your piriformis muscle attaches from the lowest part of your spine (sacrum) and travels across to your hip. The muscle helps to rotate your leg outward when it contracts. In most people, the sciatic nerve travels deep to the piriformis muscle.

When your piriformis muscle is irritated or goes into spasm, it may cause a painful compression of your sciatic nerve. Approximately ¼ of the population is more likely to suffer from piriformis syndrome because their sciatic nerve passes through the muscle.
Piriformis syndrome may begin suddenly as a result of an injury or may develop slowly from repeated irritation. Common causes include: a fall onto the buttocks, catching oneself from a “near fall,” strains, long distance walking, stair climbing or sitting on the edge of a hard surface or wallet. In many cases, a specific triggering event cannot be pinpointed. The condition is most common in 40-60 year olds and affects women more often than men.
Symptoms of piriformis syndrome include pain, numbness or tingling that begins in your buttock and radiates along the course of your sciatic nerve toward your foot. Symptoms often increase when you are sitting or standing in one position for longer than 15-20 minutes. Changing positions may help. You may notice that your symptoms increase when you walk, run, climb stairs, ride in a car, sit cross-legged or get up from a chair.
Sciatic arising from piriformis syndrome is one of the most treatable varieties and generally is relieved by the type of treatment provided in this office. You may need to temporarily limit activities that aggravate the piriformis muscle, including hill and stair climbing, walking on uneven surfaces, intense downhill running or twisting and throwing objects backwards, i.e., firewood. Be sure to avoid sitting on one foot and take frequent breaks from prolonged standing, sitting and car rides. You may find relief by applying an ice pack to your buttock for 15-20 minutes at a time, several times throughout the day.
Trigger points in the gluteus minimus
The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Lower Crossed Syndrome

Your posture plays an important role in your overall health. Poor posture leads to chronic strain and discomfort. “Lower crossed syndrome” is poor posture that results from excessive tightness in your lower back and hip flexor muscles with weakness in your abdominal and buttock muscles. Patients with lower crossed syndrome often have a “sway back.” Patients who sit for prolonged periods of time are at greater risk of lower crossed syndrome.
This postural problem commonly leads to painful conditions involving the back or hips. Successful treatment of lower cross syndrome involves stretching excessively tight muscles, strengthening weak muscles, taking frequent breaks from sitting, and modifying your workstation to be more user friendly.
Foot Over Pronation

The normal walking or running cycle begins with your heel striking the ground. As you transfer your body weight onto the front part of your foot, the arch of your foot naturally flattens slightly. This is called pronation.
The tissues that help maintain the arch of your foot are exposed to tremendous stress and may eventually break down. The loss of the normal arch of your foot results in a condition called “overpronation” or flat feet. This condition most commonly develops over a long period of time from repetitive stress.
Overpronation by itself is not painful, but the problem often leads to secondary problems, which may be painful. Plantar fasciitis, foot pain, shin splints and problems in the knee, hip or lower back are all related to overpronation. Patients who carry excess weight are more likely to develop this condition.
To help support your foot, you should wear shoes with good arch supports consistently. In some cases, specially molded orthotics may be needed to help support your arch.
What Is Upper Crossed Syndrome?
Your posture plays an important role in your overall health. Poor posture leads to chronic strain and discomfort. “Upper crossed syndrome” describes poor posture that results from excessive tightness in your shoulders and chest with weakness in your neck and mid-back. This combination forces your shoulders to roll inward and your head to project forward.

To help understand how upper crossed syndrome causes trouble, think of your spine as a telephone pole and your head as a bowling ball that sits on top. When the bowling ball is positioned directly over the top of the upright post, very little effort is required to keep it in place. If you tip the post forward and the ball begins to roll over the edge of the post, significantly more effort would be required from the muscles trying to hold it there. This effort results in chronic strain of the muscles of your neck and upper back.
The chronic strain is uncomfortable and may also lead to neck pain, upper back pain, headaches, TMJ pain, and ultimately- arthritis. This postural problem is exceptionally common in computer workstation users. Correction of this problem is accomplished by stretching the tight muscles, strengthening weak muscles, and modifying your workstation.
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
Posterior Tibial Tendon Dysfunction
|
The posterior tibialis muscle begins deep in your calf. The muscle is connected to the arch of your foot by a tendon that runs along the inside of your ankle, just behind the large bump called the medial malleolus. When you walk, the posterior tibialis muscle lifts the arch of your foot.
Posterior tibial tendon dysfunction is one of the most common foot and ankle problems. The tendon may be damaged from an acute injury, like an accident or fall. More commonly, problems arise from overuse or repeated strain. Ongoing irritation slowly damages the tendon’s fibers and eventually leads to weakening and degeneration. This decreases the tendon’s ability to support your foot when you walk. As the tendon becomes less effective, the arch of your foot is allowed to collapse, which further increases the strain on the muscle and tendon.  The condition is often triggered from overuse and/or training on excessively hard surfaces. Other factors that can contribute to posterior tibial tendon dysfunction include: obesity, diabetes, hypertension, prior surgery or steroid injections. Symptoms include pain or swelling along the course of the tendon, particularly behind your inner ankle bone. Symptoms often begin following an increase in training intensity or duration. Standing, walking, or running will likely increase your discomfort. Your pain may be aggravated by spending prolonged periods of time on your feet, especially, when standing tiptoe and walking stairs or uneven surfaces. Early diagnosis and treatment is important to slow progression of the disorder. You may need to temporarily limit weight-bearing activity to allow your tendon to heal. Using a stationary cycle, elliptical machine, or swimming can be good alternatives to walking and running. Your doctor will likely prescribe arch supports or orthotics to help support your foot. You will be given exercises to strengthen the posterior tibialis muscle. These exercises should be performed while wearing shoes with good arch supports. In certain instances, a walking cast or boot may be needed to temporarily protect your foot. |
||
|
Here is a brief description of the treatments we may use to help manage your problem.  Joint Manipulation
Your chiropractor has found joints in your body that are not moving freely. This can cause tightness and discomfort and can accelerate unwanted degeneration i.e. arthritis. Your chiropractor will apply a gentle force with their hands, or with hand held instruments, in order to restore motion to any “restricted” joints. Sometimes a specialized table will be used to assist with these safe and effective “adjustments”. Joint manipulation improves flexibility, relieves pain and helps maintain healthy joints.
 Therapy Modalities
We may apply electrotherapy modalities that produce light electrical pulses transmitted through electrodes placed over your specific sites of concern. These comfortable modalities work to decrease your pain, limit inflammation and ease muscle spasm. Hot or cold packs are often used in conjunction, to enhance the effect of these modalities. Another available option is therapeutic ultrasound. Ultrasound pushes sound vibrations into tissues. When these vibrations reach your deep tissues, heat develops and unwanted waste products are dispersed.
 Myofascial Release
Overworked muscles often become tight and develop knots or “trigger points”. Chronic tightness produces inflammation and swelling that ultimately leads to the formation of “adhesions” between tissues. Your chiropractor will apply pressure with their hands, or with specialized tools, in order to release muscle tightness and soft-tissue adhesions. This will help to improve your circulation, relieve pain and restore flexibility.
 Therapeutic Exercise
Muscle tightness or weakness causes discomfort and alters normal joint function, leading to additional problems. Your chiropractor will target tight or weak muscles with specific therapeutic stretching and strengthening to help increase tissue flexibility, build strength, and ease pain. Healthy, strong, and flexible muscles may help prevent re-injury.
 Elastic Therapeutic Tape
Your chiropractor may apply a special elastic therapeutic tape in order to support injured areas or encourage better movement. This tape is thought to decrease pain and swelling, improve circulation and limit muscle soreness.
 Foot Evaluation
Fallen arches and faulty foot mechanics are common problems that can perpetuate your condition. Our office will carefully evaluate your feet and consider the need for a change in shoe style, arch supports or even custom orthotics.
 Ankle Brace
Our office may recommend using a support brace to protect your ankle from further injury. Your doctor will discuss the specific type of brace and provide instructions for use.
|
||
|
After this initial course of treatment we will reassess your progress. We will determine the need for any additional care after your reassessment.
|
||
 Sleep Posture
Your mattress and the position you sleep in may affect your condition.
✓ Choose a mattress that provides medium or firm support, such as a traditional coil spring or adjustable airbed. Avoid waterbeds, thick pillow tops and soft, sagging mattresses. ✓ Always sleep on your back with a pillow either underneath your knees or on your side with a pillow between your knees. Avoid sleeping on your stomach. ✓ Keep your neck and back covered while sleeping to avoid drafts that could cause potential muscle spasms.  RICE
The acronym RICE can help you remember what to do after a new injury:
✓ Rest – Limit stress to the injured area for at least the first 48 hours. ✓ Ice – Apply for 10-15 minutes. Break for 30 minutes. Reapply. (Alternatives to the ice pack include Ziploc bags filled with ice, or a bag of frozen vegetables.) ✓ Compression – Wrap the injured area with an elastic ACE bandage if possible. ✓ Elevation – Elevate the injured area to limit swelling.  Standing
To avoid extra stress on your spine while standing:
✓ Avoid high-heeled shoes or boots ✓ Use a footrest ✓ If excessive standing can’t be avoided, consider shock absorbent shoes or an anti-fatigue mat.  Footwear
Improperly supported feet can affect the alignment of all of the structures above. To improve your overall comfort:
✓ Choose shoes with good arch support. ✓ Avoid going barefoot or wearing shoes that lack support (i.e. flip-flops). The following brands of sandals provide better than average arch support: Naot, Fit Flops, Orthoheels, Abeo, Vionic and Yellow box. ✓ Avoid high-heeled shoes or boots (keep heels to a maximum of 1½ inches, especially if you are going to be doing a lot of walking). ✓ “Cross-trainer” athletic shoes tend to provide the best all around support and shock absorption for daily activities. ✓ Patients with fallen arches should consider adding arch supports or orthotics. ✓ Repair or replace shoes with worn soles or heels.  Running Shoes
Running shoes need to be replaced every 250 miles. There are three basic options:
✓ Motion Control Shoes – Designed for people with low or no arches, these shoes are for runners who strike the ground on the outer edge of their foot. Avoid overly stiff shoes as these decrease you perception of ground strike and lead to new injuries. ✓ Stability or Neutral Shoes – Designed for people with normal or average arches and running mechanics. The shoe contains some cushioning to absorb shock and prevent injuries and some rigidity to avoid pronation. ✓ Cushioned Shoes – Designed for people with high arched feet. Their footprint will typically leave a thin band along the foot’s edge. As they run weight is distributed from heel strike to the outer edge of the foot and small toes that bear the brunt of “lift off.” This shoe is more flexible and absorbs the shock created by the lack or rotation (under-pronation) created by their running style. |
||
