
Some things to consider if you’re suffering from back pain.
Reasons you’re probably suffering from back pain (besides sitting all day)
Some things to consider if you’re suffering from back pain.
Reasons you’re probably suffering from back pain (besides sitting all day)

Moving is good for your back and muscles, especially if you have back pain. Check out this link for more info!
http://www.theitem.com/stories/exercise-to-help-relieve- your-lower-back-pain,296073

The muscles of the hip provide not only local stability, but also play an important role in spinal and lower extremity functional alignment. (1-4) While weakness in some hip muscles (hip extensors and knee extensors) is well tolerated, weakness or imbalance in others can have a profound effect on gait and biomechanical function throughout the lower half of the body. (5) Weakness of the hip abductors, particularly those that assist with external rotation, has the most significant impact on hip and lower extremity stability. (5,6)

The gluteus medius is the principal hip abductor. When the hip is flexed, the muscle also assists the six deep hip external rotators (piriformis, gemelli, obturators, and quadratus femoris). The gluteus medius originates on the ilium just inferior to the iliac crest and inserts on the lateral and superior aspects of the greater trochanter. While the principal declared action of the gluteus medius is hip abduction, clinicians will appreciate its more valuable contribution as a dynamic stabilizer of the hip and pelvis- particularly during single leg stance activities like walking, running, and squatting. The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance. The remainder comes predominantly from 2 muscles that insert onto the iliotibial band: the tensor fascia lata and upper gluteus maximus. Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity. (6)
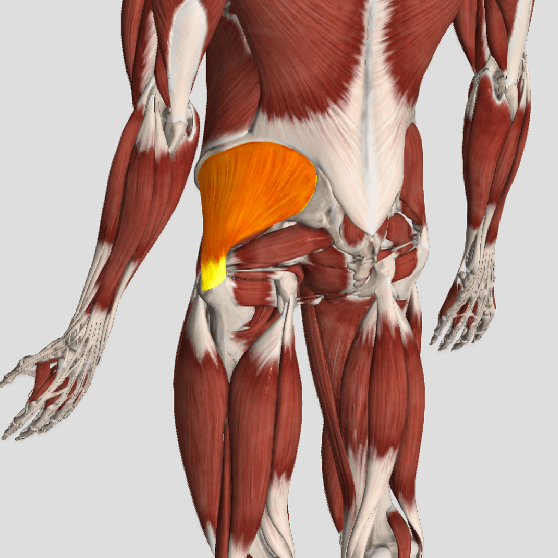
Incompetent hip abductors and/or external rotators allows for excessive adduction and internal rotation of the thigh during single leg stance activities. This leads to a cascade of biomechanical problems, including pelvic drop, excessive hip adduction, excessive femoral internal rotation, valgus knee stress, and internal tibial rotation. (1,7-12)
By Bryan Cobb, Advanced Remedial Massage Therapist

What is a Trigger Point?
Trigger Points (TP’s) are defined as a “hyper-irritable spot within a taut band of skeletal muscle. The spot is painful on compression and can evoke characteristic referred pain and autonomic phenomena.”1
Put into plain language, a TP is a painful knot in muscle tissue that can refer pain to other areas of the body. You have probably felt the characteristic achy pain and stiffness that TP’s produce, at some time in your life.
TP’s were first brought to the attention of the medical world by Dr. Janet G. Travell. Dr. Travell, physician to President John F. Kennedy, is the acknowledged Mother of Myofascial Trigger Points. In fact, “Trigger Point massage, the most effective modality used by massage therapists for the relief of pain, is based almost entirely on Dr. Travell’s insights.”2 Dr. Travell’s partner in her research was Dr. David G. Simons, a research scientist and aerospace physician.
Trigger Points are very common. In fact, Travell and Simons state that TP’s are responsible for, or associated with, 75% of pain complaints or conditions.1 With this kind of prevalence, it’s no wonder that TP’s are often referred to as the “scourge of mankind”.
Trigger Points can produce a wide variety of pain complaints. Some of the most common are migraine headaches, back pain, and pain and tingling into the extremities. They are usually responsible for most cases of achy deep pain that is hard to localize.
A TP will refer pain in a predictable pattern, based on its location in a given muscle. Also, since these spots are bundles of contracted muscle fibres, they can cause stiffness and a decreased range of motion. Chronic conditions with many TP’s can also cause general fatigue and malaise, as well as muscle weakness.
Trigger Points are remarkably easy to get, but the most common causes are
TP’s (black X) can refer pain to other areas (red)
Sudden overload of a muscle
Once in place, a TP can remain there for the remainder of your life unless an intervention takes place.
Trigger Points Not Well Known
With thousands of people dealing with chronic pain, and with TP’s being responsible for — or associated with — a high percentage of chronic pain, it is very disappointing to find that a large portion of doctors and other health care practitioners don’t know about TP’s and their symptoms.
Scientific research on TP’s dates back to the 1700’s. There are numerous medical texts and papers written on the subject.
But, it still has been largely overlooked by the health care field. This has led to needless frustration and suffering, as well as thousands of lost work hours and a poorer quality of life.
How Are Trigger Points Treated?
As nasty and troublesome as TP’s are, the treatment for them is surely straight-forward. A skilled practitioner will assess the individual’s pain complaint to determine the most likely location of the TP’s and then apply one of several therapeutic modalities, the most effective of which is a massage technique called “ischemic compression”.
Basically, the therapist will apply a firm, steady pressure to the TP, strong enough to reproduce the symptoms. The pressure will remain until the tissue softens and then the pressure will increase appropriately until the next barrier is felt. This pressure is continued until the referral pain has subsided and the TP is released. (Note: a full release of TP’s could take several sessions.)
Other effective modalities include dry needling (needle placed into the belly of the TP) or wet needling (injection into the TP). The use of moist heat and stretching prove effective, as well. The best practitioners for TP release are Massage Therapists, Physiotherapists, and Athletic Therapists. An educated individual can also apply ischemic compression to themselves, but should start out seeing one of the above therapists to become familiar with the modality and how to apply pressure safely.
1 Simons, D.G., Travell, D.G., & Simons, L.S. Travell and Simons’Myofascial Pain and Dysfunction: the Trigger Point Manual.
Vol. 1. 2nd ed. Lippincott, Williams, and Wilkins, 1999.
Great article – thanks to Dr. C. Liebenson for the share.
From the Journal Pain Physician: Incidence of Spontaneous Resorption of
Lumbar Disc Herniation: A Meta-Analysis.
Due to the natural course of lumbar disc herniations (LDH) patients should consider conservative treatment before surgery.
“There is a general consensus among contemporary orthopedists
that, for most patients with LDH, an initial
trial of conservative treatment is preferable to surgical
intervention.”
Source: Zhong, M., et al. (2017). Incidence of Spontaneous Resorption of Lumbar Disc Herniation: A Meta-Analysis. Pain Physician, 20, E45-E52

In a nation of only 36 million people, over 5 million people turned to opioid use for their pain despite the availability of better options. Opioids should never be the first step in pain management; preventing overuse takes education of both the public who are using and the professionals prescribing these drugs.
At Aberdeen Chiropractic we are proud to be part of the solution to Canada’s opioid crisis by providing safe, effective care for back pain, neck pain and headaches. Our goal is to assess, correct and prevent your pain with a variety of interventions including Chiropractic, Acupuncture, Laser, Exercise Rehabilitation and Trigger Point Therapy.


Happy #WorldSpineDay !!!
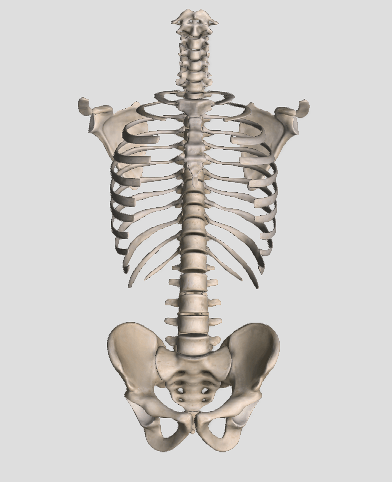
The spine is made up of 24 bones, called vertebrae. Ligaments and muscles connect these bones together to form the spinal column. The spinal column gives the body form and function. The spinal column holds and protects the spinal cord, which is a bundle of nerves that sends signals to other parts of the body.
.
.
.
.
.
.
.
.
#Chiropractic
#Spine
#Health
#fitness
#chiropractor

The muscle responsible for flexing your hip toward your trunk, is called the Psoas. This muscle begins on your lower spine and passes through your pelvis to attach onto the top of your femur (thigh bone). Along this course, the muscle travels across the front of your hip socket and over several bony prominences. If the muscle is too tight, its tendon may rub over these “bumps”. This occasionally produces an audible snapping sound, hence the moniker, “snapping hip”, aka “psoas tendinopathy”.
The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
Your symptoms may include a “snapping” sound or sensation when you flex and extend your hip- although many cases are silent. Repeated rubbing causes inflammation and subsequent deep groin pain that can radiate to the front of your hip or thigh. Long-standing problems can trigger weakness or even limping.
The diagnosis of snapping hip is frequently overlooked. In fact, some studies show that identification is often delayed more than two years, while other potential causes are pursued. Fortunately, your problem has been recognized, and our office has several treatments to help you recover.
Psoas problems often start when one group of muscles is too tight, while another is too loose. Your home exercises will help to correct this problem. Depending upon the severity of your condition, you may need to avoid certain activities for a while. You should especially avoid repetitive hip flexion. Prolonged seated positions can encourage shortening of your hip flexors so be sure to take frequent breaks. Patients with fallen arches may benefit from arch supports.
If you or someone you know suffers from this condition, call our office today. Our doctors are experts at relieving many types of pain including hip injuries.
