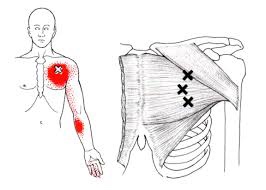
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Winnipeg
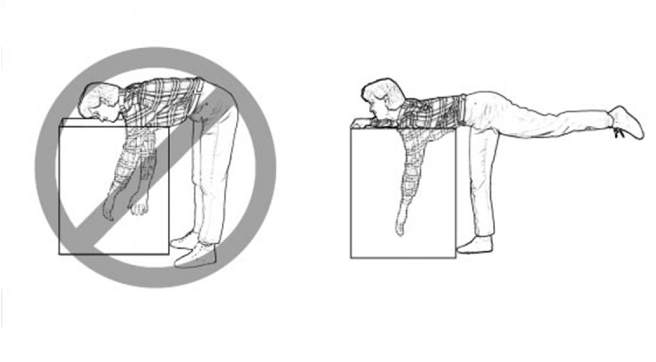
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
CTS at Night.
For those who have carpal tunnel syndrome (CTS), it’s no surprise that CTS is frequently most expressive during the night, often to the point of interrupting sleep and/or making it difficult to fall back to sleep. So why is that?
The primary reason for nighttime CTS symptoms has to do with the wrist, as it is very difficult to sleep with the wrist held in its “ideal” or least irritating position. In fact, most people favor “curling” the back of the hand under the chin or bending the hand/wrist backwards under the head. When the wrist is bent in either direction, it can increase the pressure inside the wrist, which can generate the various symptoms associated with CTS.
One study evaluated the pressure inside the carpal tunnel while participants slowly moved their wrists. The researchers found many movements didn’t need to exceed 20 degrees before the pressure increased enough within the carpal tunnel to generate symptoms.
Because it doesn’t take a lot of movement to build up excessive pressure in the wrists of those with CTS, many doctors recommend the use of a “cock-up splint” for the non-surgical treatment of CTS in order to help keep the wrist in a neutral position.
Wrist posture is also an important factor during the day. One study looked at typing on a tablet PC, which allowed people to work in non-traditional settings. As screen size reduced, the posture required to type became more limited and accelerated the usual rate of pain onset in the neck, elbows, and wrists.
This study also looked at three different positions used when working on touch-screen devices: desk, lap, and bed. The healthy subjects completed six, 60-minute typing sessions using three virtual keyboard designs: standard, wide, and split. The researchers monitored the position of the wrist, elbow, and neck while the participants typed and followed up each session with questionnaires designed to measure discomfort.
The research team reported that typing in bed required greater wrist extension but resulted in a more natural elbow position than typing at a desk. The angled split keyboard significantly reduced the wrist deviation vs. the standard or wide keyboard designs. All three regions—the neck, elbow, and wrist—exhibited more movements (13% to 38%) towards the end of the one hour sessions, which correlated with a significant increase in pain in every body region investigated. Overall, using a wider keyboard while sitting at a desk was the most tolerable position among study participants.

Trigger points in the rhomboid muscles.
This is another common muscle to get trigger points. It originates on the spinous processes of the T2-T5 vertebrae. It inserts on the medial border of the scapula. It’s main actions are to adduct the scapula pulling it back toward the spine, and to rotate the glenohumeral joint downward. This muscle also prevents wining of the scapula. This muscle is often overloaded by a sitting posture where the shoulders are rolled forward such as when using a computer. The Rhomboids are often weak and under trained in people. Trigger points in this muscle cause pain and ache in the upper back between the shoulder blade. Strength trading for this muscle is necessary to help prevent postural overload. 
When Are My Shoes “Done”?

Running shoes need to be replaced every 250 miles. There are three basic options:
✓ Motion Control Shoes – Designed for people with low or no arches, these shoes are for runners who strike the ground on the outer edge of their foot. Avoid overly stiff shoes as these decrease you perception of ground strike and lead to new injuries.
✓ Stability or Neutral Shoes – Designed for people with normal or average arches and running mechanics. The shoe contains some cushioning to absorb shock and prevent injuries and some rigidity to avoid pronation.
✓ Cushioned Shoes – Designed for people with high arched feet. Their footprint will typically leave a thin band along the foot’s edge. As they run weight is distributed from heel strike to the outer edge of the foot and small toes that bear the brunt of “lift off.” This shoe is more flexible and absorbs the shock created by the lack or rotation (under-pronation) created by their running style.
How long does Whiplash last?

First, what is whiplash? It’s a lot of things, which is why the term WAD or Whiplash Associated Disorders has become the most common term for the main signs and symptoms associated with a whiplash injury. WAD is usually associated with a motor vehicle collision, but sports injuries, diving accidents, and falls are other common ways to sustain a WAD injury.
To answer the question of the month, in most cases, the recovery rate is high and favors those who resume their normal daily activities. The worse thing you can do when you sustain a WAD injury is to not do anything! Too much rest and inactivity leads to long-term disability. Of course, this must be balanced with the degree of injury, but even when the injury requires some “down time,” stay as active as possible during the healing phase.
Many people recover within a few days or weeks while a smaller percentage require months and about 10% may only partially recover. So what can be done to give you the best possible chance to fully recover as soon as possible?
During recovery, you can expect your condition to fluctuate in intensity so “listen” to your body, let it “guide” you during activity and exercise, and stay within “a reasonable boundary of pain” during your activity. Remember, your best chance for full recovery FAVORS continuing a normal lifestyle. Make reasonable modifications so you can work, socialize, and do your “normal” activities!
The KEY: Stay in control of your condition – DO NOT let it control you! Here are some tips:
1) POSTURE CONTROL: Keep the weight of the head back by gliding your chin back until you “hit” a firm end-point. Then release it slightly so it’s comfortable—this is your NEW head position!
2) FLEXIBILITY: Try this range of motion (ROM) exercise… Slowly flex your neck forwards and then backwards, then bend your neck to the left and then the right, and then rotate it to the left and to then to the right. THINK about each motion and avoid sharp, knife-like pain; a “good-hurt” is okay! Next, do the same thing with light (one-finger) resistance in BOTH directions. Try three slow reps four to six times a day!
3) MUSCLE STRENGTH: Try pushing your head gently into your hand in the six directions listed above to provide a little resistance. Next, reach back with both hands or wrap a towel around your neck and pull forwards on the towel while you push the middle of your neck backwards into the towel doing the chin-tuck/glide maneuver (same as #1). Repeat three to five times slowly pushing, and more importantly, release the push slower! This is the MOST IMPORTANT of the strengthening exercises in most cases! Next, “squeeze” your shoulder blades together followed by spreading them as far apart as possible (repeat three to five times).
4) PERIODIC BREAKS: Set a timer to remind yourself to do a stretch, get up and move, to tuck your chin inwards (#1) and do some of #2 and #3 every 30-60 minutes.
5) LIFTING/CARRYING/WORK: Be SMART! Do not re-injure yourself. Change the way you handle yourself in your job, in the house, and while performing recreational activities.
6) HOUSEHOLD ACTIVITIES: Use a dolly to move boxes and keep commonly used items within easy reach (not too high or low).
Be smart, stay educated, work within the range your body tells you is “safe” and most importantly, STAY IN CONTROL!!!
My back hurts, why look at my feet?
Improperly supported feet can affect the alignment of all of the structures above. To improve your overall comfort:
✓ Choose shoes with good arch support.
✓ Avoid going barefoot or wearing shoes that lack support (i.e. flip-flops). The following brands of sandals provide better than average arch support: Naot, Fit Flops, Orthoheels, Abeo, Vionic and Yellow box.
✓ Avoid high-heeled shoes or boots (keep heels to a maximum of 1½ inches, especially if you are going to be doing a lot of walking).
✓ “Cross-trainer” athletic shoes tend to provide the best all around support and shock absorption for daily activities.
✓ Patients with fallen arches should consider adding arch supports or orthotics.
✓ Repair or replace shoes with worn soles or heels.
Lifting Mechanics Made Simple

Here are some tips to help you lift safely:
✓ Avoid lifting or flexing before you’ve had the chance to warm up your muscles (especially when you first awaken or after sitting or stooping for a period of time).
✓ To lift, stand close directly facing object with your feet shoulder width apart.
✓ Squat down by bending with your knees, not your back. Imagine a fluorescent light tube strapped to your head and hips when bending. Don’t “break” the tube with improper movements. Tuck your chin to help keep your spine aligned.
✓ Slowly lift by thrusting your hips forward while straightening your legs.
✓ Keep the object close to your body, within your powerzone” between your hips and chest. Do not twist your body, if you must turn while carrying an object, reposition your feet, not your torso.
An alternative lifting technique for smaller objects is the golfers lift. Swing one leg directly behind you. Keep your back straight while your body leans forward. Placing one hand on your thigh or a sturdy object may help.
How can a low speed crash cause injury?
There is certainly a lot of interest in concussion these days between big screen movies, football, and other sports-related injuries. Concussion, traumatic brain injury (TBI), and mild traumatic brain injury (mTBI) are often used interchangeably. Though mTBI is NOT the first thing we think about in a low-speed motor vehicle collision (MVC), it does happen. So how often do MVC-related TBIs occur, how does one know they have it, and is it usually permanent or long lasting?
Here are some interesting statistics: 1) The incidence rate of fatal and hospitalized TBI in 1994 was estimated to be 91/100,000 (~1%); 2) Each year in the United States, for every person who dies from a brain injury, five are admitted to hospitals and an additional 26 seek treatment for TBI; 3) About 80% of TBIs are considered mild (mTBI); 4) Many mTBIs result from MVCs, but little is known or reported about the crash characteristics. 5) The majority (about 80%) of mTBI improve within three months, while 20% have symptoms for more than six months that can include memory issues, depression, and cognitive difficulty (formulating thought and staying on task). Long-term, unresolved TBI is often referred to as “post-concussive syndrome.”
In one study, researchers followed car crash victims who were admitted into the hospital and found 37.7% were diagnosed with TBI, of which the majority (79%) were defined as minor by a tool called Maximum Abbreviated Injury Scale (MAIS) with a score of one or two (out of a possible six) for head injuries. In contrast to more severe TBIs, mild TBIs occur more often in women, younger drivers, and those who were wearing seatbelts at the time of the crash. Mild TBI is also more prevalent in frontal vs. lateral (“T-bone”) crashes.
As stated previously, we don’t think about our brains being injured in a car crash as much as we do other areas of our body that may be injured—like the neck. In fact, MOST patients only talk about their pain, and their doctor of chiropractic has to specifically ask them about their brain-related symptoms.
How do you know if you have mTBI? An instrument called the Traumatic Brain Injury Questionnaire can be helpful as a screen and can be repeated to monitor improvement. Why does mTBI persist in the “unlucky” 20%? Advanced imaging has come a long way in helping show nerve damage associated with TBI such as DTI (diffuse tensor imaging), but it’s not quite yet readily available. Functional MRI (fMRI) and a type of PET scanning (FDG-PET) help as well, but brain profusion SPECT, which measures the blood flow within the brain and activity patterns at this time, seems the most sensitive.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honored to render our services.
A Few Sleep Tips From Us To You

Your mattress and the position you sleep in may affect your spine.
✓ Choose a mattress that provides medium or firm support, such as a traditional coil spring or adjustable airbed. Avoid waterbeds, thick pillow tops and soft, sagging mattresses.
✓ Always sleep on your back with a pillow either underneath your knees or on your side with a pillow between your knees. Avoid sleeping on your stomach.
✓ Keep your neck and back covered while sleeping to avoid drafts that could cause potential muscle spasms.
Here are a couple of tips to help you get in and out of bed more comfortably:
✓ To lie down: Sit on the edge of the bed, pull your arms to your sides and tilt your body into the bed, maintaining the bend of your knees at 45 degrees. Finally, bring your feet into in a lying position or roll onto your back.
✓ To get up: From a side-lying position with your knees bent, push your body upright into a sitting position, swinging your legs over the edge of the bed as you rise.
If you find that you wake up sore then you may be suffering from any number of conditions that get worse overnight.
