

Fibromyalgia (FM) is a common cause for chronic pain (pain that lasts three or more months) and afflicts 4% of the general population in the United States! FM commonly affects the muscles and soft tissues – not the joints (like arthritis); however, many FM sufferers are mistakenly diagnosed with arthritis, so it may take years before they get an accurate diagnosis. There are NO known accurate diagnostic tests for FM, which is another reason for a delayed diagnosis.
In order to answer the question, “Can fibromyalgia be prevented?” we must first find the cause of FM. There are two types of FM: PRIMARY and SECONDARY. Primary FM occurs for no known reason, while secondary FM can be triggered by a physical event such as a trauma (e.g., car accident), an emotional event or a stressful situation (e.g., loss of a child), and/or a medical event such as a condition like irritable bowel syndrome, rheumatoid arthritis, or systemic lupus erythymatosis (SLE). Any condition that carries chronic or long-lasting symptoms can trigger FM, and some argue that the lack of being able to get into the deep sleep stage may be at the core of triggering FM since sleep disorders are a common finding in FM sufferers!
The “KEY” to managing FM has consistently been and probably always will be EXERCISE and SLEEP. So, if FM is preventable, daily exercise and getting the “right kind” of sleep are very important ways that may reduce the likelihood for developing the condition! Since emotions play a KEY ROLE in the cause and/or effect of FM, applying skills that keep life’s stressors in check is also important. This list can include hobbies like reading a good book, playing and/or listening to music, or meditation. The combination of exercise with mindful meditation using approaches like Tai Chi, Yoga, Qi Gong, and others has had positive impacts on FM patients such as improved balance and stability, reduced pain, enhanced mental clarity, and generally improved quality of life. Managing physical conditions that are associated with FM (such as irritable bowel syndrome, rheumatoid arthritis, or systemic lupus erythymatosis) is also important in managing and/or preventing FM.
Another management strategy of FM is diet. As most patients with FM will agree, certain foods help and others make the FM symptoms worse. In a survey published in the Journal of Clinical Rheumatology, 42% of FM patients reported certain foods exacerbated their symptoms. Of course, each individual case is unique, so keeping a food log or journal can be very helpful to determine dietary “friends” vs. “enemies.” The first step is to eliminate certain foods for four to six weeks, such as dairy and/or gluten. Most patients report a significant improvement in energy (less fatigue) while some report less pain when problem foods are eliminated from their diet. Generally, a diet rich in fruits, vegetables, and lean proteins can have a positive impact on the FM patient. Consider eating multiple small meals vs. two or three large meals during the day, as this can keep blood sugar levels more stable and reduce fatigue.
So back to the question, can fibromyalgia be prevented? Maybe…maybe not. Since the medical community doesn’t know the exact cause, it’s hard to answer this question. However, being proactive and implementing the strategies used to better manage FM may help in preventing it as well!
If you, a friend or family member requires care for Fibromyalgia, we sincerely appreciate the trust and confidence shown by choosing our services!

Becoming healthy and staying healthy is hard, challenging work but worth every second of persistence.

https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2517920#ioi160017r18
Some very interesting findings in this study. Over the course of two years participants who were part of the fasting group showed a weight loss of 10% on average as well as improved perceptions of quality of life, energy, sleep quality and libido.
Is fasting right for you? That depends and it is an idea that you and your health care professional should discuss as what works for some may not be right for you.
By Bryan Cobb, Advanced Remedial Massage Therapist

What is a Trigger Point?
Trigger Points (TP’s) are defined as a “hyper-irritable spot within a taut band of skeletal muscle. The spot is painful on compression and can evoke characteristic referred pain and autonomic phenomena.”1
Put into plain language, a TP is a painful knot in muscle tissue that can refer pain to other areas of the body. You have probably felt the characteristic achy pain and stiffness that TP’s produce, at some time in your life.
TP’s were first brought to the attention of the medical world by Dr. Janet G. Travell. Dr. Travell, physician to President John F. Kennedy, is the acknowledged Mother of Myofascial Trigger Points. In fact, “Trigger Point massage, the most effective modality used by massage therapists for the relief of pain, is based almost entirely on Dr. Travell’s insights.”2 Dr. Travell’s partner in her research was Dr. David G. Simons, a research scientist and aerospace physician.
Trigger Points are very common. In fact, Travell and Simons state that TP’s are responsible for, or associated with, 75% of pain complaints or conditions.1 With this kind of prevalence, it’s no wonder that TP’s are often referred to as the “scourge of mankind”.
Trigger Points can produce a wide variety of pain complaints. Some of the most common are migraine headaches, back pain, and pain and tingling into the extremities. They are usually responsible for most cases of achy deep pain that is hard to localize.
A TP will refer pain in a predictable pattern, based on its location in a given muscle. Also, since these spots are bundles of contracted muscle fibres, they can cause stiffness and a decreased range of motion. Chronic conditions with many TP’s can also cause general fatigue and malaise, as well as muscle weakness.
Trigger Points are remarkably easy to get, but the most common causes are
TP’s (black X) can refer pain to other areas (red)
Sudden overload of a muscle
Once in place, a TP can remain there for the remainder of your life unless an intervention takes place.
Trigger Points Not Well Known
With thousands of people dealing with chronic pain, and with TP’s being responsible for — or associated with — a high percentage of chronic pain, it is very disappointing to find that a large portion of doctors and other health care practitioners don’t know about TP’s and their symptoms.
Scientific research on TP’s dates back to the 1700’s. There are numerous medical texts and papers written on the subject.
But, it still has been largely overlooked by the health care field. This has led to needless frustration and suffering, as well as thousands of lost work hours and a poorer quality of life.
How Are Trigger Points Treated?
As nasty and troublesome as TP’s are, the treatment for them is surely straight-forward. A skilled practitioner will assess the individual’s pain complaint to determine the most likely location of the TP’s and then apply one of several therapeutic modalities, the most effective of which is a massage technique called “ischemic compression”.
Basically, the therapist will apply a firm, steady pressure to the TP, strong enough to reproduce the symptoms. The pressure will remain until the tissue softens and then the pressure will increase appropriately until the next barrier is felt. This pressure is continued until the referral pain has subsided and the TP is released. (Note: a full release of TP’s could take several sessions.)
Other effective modalities include dry needling (needle placed into the belly of the TP) or wet needling (injection into the TP). The use of moist heat and stretching prove effective, as well. The best practitioners for TP release are Massage Therapists, Physiotherapists, and Athletic Therapists. An educated individual can also apply ischemic compression to themselves, but should start out seeing one of the above therapists to become familiar with the modality and how to apply pressure safely.
1 Simons, D.G., Travell, D.G., & Simons, L.S. Travell and Simons’Myofascial Pain and Dysfunction: the Trigger Point Manual.
Vol. 1. 2nd ed. Lippincott, Williams, and Wilkins, 1999.

Evidence-based chiropractors must routinely answer two questions:
Chiropractors treat the cause of dysfunction and not the just the pain—right? This becomes more challenging when patients present with an assortment of orthopedic diagnoses. Let’s be honest, we see the worst of the worst on a daily basis, and we are often the last option.
Identifying IF inflammation is a source of pain may be one of the biggest differentiators in your initial exam.
Chiropractors see patients in pain resulting from acute injuries. Newly injured tissue often contains an inflammatory component for healing. However, emerging clinical research tells us that reoccurring painful conditions often lack an inflammatory component. Effective treatment of pain is dependent on a clear understanding of whether inflammation is present or not.
Learn how to identify chemical vs. mechanical pain
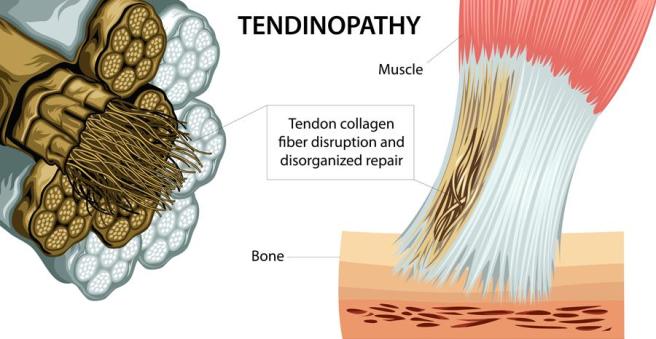
Many chronic tendon problems are not the result of ongoing inflammation, rather failed inflammation. Chronic failed inflammation results in tissue degeneration that diminishes long-term tissue capacity, size, and function. Tendons, when degenerated, exhibit lower stiffness. A failed healing response results in proliferation of tissue with decreased load transfer and elastic capability. We sometimes refer to this as scar tissue. This deficit must be accounted for during locomotion. Diminished tendon load transfer will lead to widespread biomechanical dysfunction. The patient must be willing to change their movement pattern or habits to stop this process.
Chronic problems often lead to widespread biomechanical dysfunction.
We have all seen the patient with chronic, but intermittent, plantar fasciitis who develops subsequent knee, hip, or back pain. Human movement is coordinated by a hierarchal system. The CNS initiates, controls and executes movement patterns. The human body knows movements—not muscles. If one tissue in the loop loses its integrity the patient may develop a new movement pattern. This new movement pattern may not be efficient to all the tissue components and result in new injuries. Our tissue only has a certain capacity. Muscles and tendons will strain, ligaments will sprain, and bones will break at different rates and/or amounts of load. Rehab should focus on optimal movement patterns instead of strengthening isolated muscles.
Let’s examine a patient with Achilles tendinosis?
Patients with Achilles pain will often favor the outside of their foot. Pain will result in an adaptive behavior altering the activity of agonist, synergist and antagonist muscles. A recent study in the Journal of Physiology highlighted this compensatory behavior:
“This was seen during single-legged hopping, where the contribution from the triceps surae muscle to the plantar flexors was decreased and the co-contraction from the tibialis anterior muscle was also decreased on the involved side in individuals with Achilles tendinosis. This may be attributed to the protective mechanism shielding the already injured tendon from further injury or even rupture.” (1)
If the agonist and antagonists have decreased activity, then how do these patients transfer load while walking?
“The EMG activity of the synergist muscle, the peroneal longus muscle in the present study, increased to compensate for the mechanical deficit resulting from the compliant Achilles tendon and to achieve the task goal.”
These patients have now condemned their gait cycle to walk on a supinated foot that transfers compensatory repercussions to the knee and hip. The increased load on the peroneal muscles may also result in injury in time. This is not an isolated problem, rather the typical continuum of an “…itis” to an “…opathy” over time. These are not isolated lesions; rather the start of widespread biomechanical dysfunction that may result in any number of orthopedic diagnosis. The authors conclude:
“Pain is a signal of tissue damage, although damaged tissues are not always painful.”
Excellent chiropractic clinical outcomes require that providers look upstream and downstream for biomechanical co-conspirators. ChiroUp helps your patients recognize how specific orthopedic conditions change movement patterns. Preselected exercise protocols incorporate ideal movement patterns during the rehab process. In the case of tendinopathy, ChiroUp protocols incorporate eccentric exercise to facilitate and strengthen the damaged tissue and prevent recurrence of pain.
Reference

Headaches can arise from many different causes. A partial list includes stress, lack of sleep, allergies, neck trauma (particularly sports injuries and car accidents), and more. In some cases, the cause may be unknown.
A unique common denominator of headaches has to do with cervical spine anatomy, in particular the upper part of the neck. There are seven cervical vertebrae, and the top three (C1-3) give rise to three nerves that travel into the head. These nerves also share a pain nucleus with the trigeminal nerve (cranial nerve V), which can route pain signals to the brain.
Depending on which nerve is most irritated, the location of the headache can vary. For example, C2—the greater occipital nerve—travels up the back of the head to the top. From there, it can communicate with another nerve (cranial nerve V or the trigeminal nerve), which can refer pain to the forehead and/or behind the eye.
When C1—the lesser occipital nerve—is irritated, pain travels to the back of the head, while irritation to C3—the greater auricular nerve—results in pain to an area just above the ear. When a nerve is pinched, the altered sensation can include pain, numbness, tingling, burning, itching, aching, or a combination of these sensations.
These are classified as cervicogenic headaches (CGH), and as the name implies, the origin of pain/altered sensation arises from the neck.
A 2013 study reviewing the literature on CGH found that manipulation and mobilization improved pain, disability, and function. The most effective approach included manipulation combined with neck-upper back strengthening exercises.
But what about migraine headaches? Migraines are vascular headaches, and some (but not all) are preceded by an aura or a pre-headache warning that may include blurry vision, tingling, strange olfactory sensations, etc. One study of 127 migraine sufferers reported fewer attacks and less medication required by those who received chiropractic care.
The good news is that spinal manipulation is very safe, and a trial is often very rewarding for many types of headaches.
Carpal tunnel syndrome (CTS) is the most common of the many “entrapment neuropathies”— nerve pinches in the arms or legs—likely because we use our hands and fingers repetitively for long time frames at work and during many of our hobbies. In addition, the wrist is a very complicated joint because it’s not a simple ball-and-socket or hinge, like the hip, elbow, or knee.
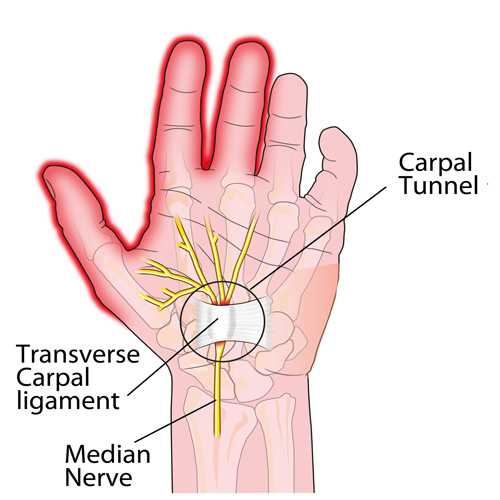
The wrist is made up of eight small “carpal” bones that are all shaped very differently and fit together a bit like a puzzle. These eight bones are lined up in two rows of four bones that form the “roof“ of the tunnel.
The shape of the tunnel changes with different activities, and the contents within the tunnel have to accommodate for this. Nine of the tendons that allow the hand to move the fingers also travel through the tunnel. Look at the palm-side of your wrist as you wiggle your fingers. See all the activity going on there? The median nerve travels through the tunnel as well, just under the “floor”, which is a very strong ligament that stretches from the pinky to the thumb-side of the tunnel.
Virtually ANY condition that increases the pressure inside the already tightly packed tunnel can create CTS symptoms like numbness, tingling, burning, etc. Over time, grip strength may weaken, causing one to accidentally drop objects.
To add to the causation list of CTS, conditions like obesity, pregnancy, diabetes, hypothyroid, rheumatoid arthritis (and other “arthropathies”), taking birth control pills (BCPs), and more can cause CTS without any increase in hand/wrist activities!
So HOW can we prevent CTS?
First, consider your job and your “workstation.” There are ergonomic keyboard and mouse options that can help you maintain a “neutral” wrist posture. If you have to bend your wrist a lot to do your work tasks—like placing items in a package, assembly work, etc.—see if you can change the angle of the package or assembly set up that allows your wrist to be straight, NOT BENT! Also, sit/stand up straight, chin tucked back, and DON’T SLOUCH!
A “night splint” forces the wrist to stay straight and can REALLY help! Managing your weight and health (manage your diabetes, thyroid, and medications that increase swelling like BCPs) is VERY important! There are also natural anti-inflammatory vitamins and herbs like ginger, turmeric, and bioflavonoid you may want to consider—your doctor of chiropractic can help you with this!
Chiropractors can manage CTS very well and can frequently help patients avoid the need for a surgical release. The “KEY” is to not wait—get treated early on!
