The deltoid is the the muscle that is most often thought of as the “shoulder.” It is the diamond shaped muscle that caps the shoulder joint. It originates on the clavicle, the acromion, and the spine of the scapula. It inserts on the deltoid tuberosity of the humerus. As a whole unit the deltoid laterally abducts the humerus at the glenohumeral joint. The anterior portion of the delt forward flexes the arm, as well as horizontally flexing the arm across the chest. Since the deltoid is involved in almost all shoulder movements it is especially prone to trigger points. Points in the anterior deltoid refer into the anterior and lateral shoulder. Trigger points in the posterior deltoid refer pain into the posterior shoulder with spillover down the lateral arm. 
Physio
He barely hit me; why does it hurt?
Error
This video doesn’t exist
You may have heard the comment, “If there’s no damage to the car, then there’s no injury.” Unfortunately, that does not always seem to be the case.
There are MANY factors that affect the dynamics of a collision and whether or not injury occurs. A short list includes: vehicle type and design, speed, angle of collision, momentum, acceleration factors, friction, kinetic and potential energy, height, weight, muscle mass, seat back angle and spring, head position upon impact, etc.
Consider Sir Isaac Newton’s Third Law of Motion: “For every action there is an equal and opposite reaction.” This law applies to a car accident at any speed. Using the analogy of hitting a pool ball into the corner pocket straight on, when the cue ball stops, its momentum is transferred to the target ball which accelerates at the same speed…hopefully into the corner pocket!
This example is not quite the same as an automobile collision because the energy transfer is very efficient due in part to the two pool balls not deforming (crushing or breaking) on impact with one another. If either ball did deform, more energy absorption would occur and the acceleration of the second ball would be lower.
In fact, in the United States, vehicle bumpers are tested at 2.5 mph with impact equipment of similar mass with the test vehicle’s brakes disengaged and the transmission in neutral. National Highway Transportation Highway Safety Administration (NHTSA) vehicle safety standards demand that no damage should occur to the car in this scenario.
However, energy transfer occurs very quickly and with a greater amount of force when there is no vehicle deformation (damage). As a result, a greater amount of energy (described as G-force) is directly transferred to the occupants inside the vehicle—increasing the risk of injury. A 1997 Society of Automobile Engineers article provided an example in which the same 25 mph (12 m/s) collision resulted in a five-times greater force on the occupants of the vehicle when the crush distance of the impact fell from 1 meter to .2 meters.
So be aware that even low-speed impacts can still place quite a bit of force on your body, even if the bumper of your car doesn’t have a scratch on it.
What is a Migraine? What can I do about them?
A “migraine” is an intense throbbing headache that may be accompanied by nausea, vomiting, and sensitivity to light or noise. Adult women are three times more likely than men to experience migraines. The frequency of migraine headaches usually peaks between age 30 and 40, and attacks decrease thereafter. The onset of a new migraine headache after age 50 is rare.
 Migraine headaches are caused by a combination of nerve irritation and enlargement of the blood vessels in your brain. Migraines tend to run in families and sufferers have inherited a sensitive nervous system from their parents. Patients who are overweight or have other vascular risk factors are more likely to suffer from migraines.
Migraine headaches are caused by a combination of nerve irritation and enlargement of the blood vessels in your brain. Migraines tend to run in families and sufferers have inherited a sensitive nervous system from their parents. Patients who are overweight or have other vascular risk factors are more likely to suffer from migraines.
Migraines are set off by “triggers” and the headache occurs when the number of triggers reaches a critical threshold. This can be likened to a glass of water that overflows at a certain point. Known triggers include: neck tightness, stress, smoking, strong odors (i.e. perfumes), bright or flickering lights, fluorescent lighting, too little or much sleep, head trauma, weather changes, motion sickness, cold (ice cream headaches), lack of activity or exercise, overexertion, fatigue, eyestrain, dehydration, hunger, fasting, and hormonal changes, including menstruation and ovulation. Certain medications, including hormones or oral contraceptives are known triggers. A detailed list of foods that trigger migraines is provided below.
About 20-33% of people who get migraines have warning symptoms, called an “aura”, before their actual headache attack. Aura symptoms develop slowly over five to 20 minutes and can last up to an hour. The most common aura is a band of absent vision with an irregular shimmering border. Some patients report numbness or tingling in their arms or face. Be sure to tell your doctor if you experience any confusion or decreased consciousness with your headache. Other signs to watch for include: abrupt headaches that develop and peak very quickly, headaches that develop following a head injury, light-headedness, dizziness, difficulty speaking, difficulty swallowing, difficulty walking, fever, rash, or any “new” headache that is significantly different from your prior headaches.
Many patients benefit from the types of treatment provided in this office. Research has shown a “significant reduction” in migraine frequency and intensity through chiropractic care. Your home management will focus on avoiding “triggers” and stress. You should begin keeping a headache diary to help you track and eliminate triggers. Patients who experience migraines are more susceptible to other types of cardiovascular disease, like heart attack and stroke. Be sure to choose a “heart healthy” diet (i.e. limit sodium and fats) and keep your weight controlled. Eat at regular intervals and stay well-hydrated as hunger and dehydration are known triggers.
Your doctor may talk to you about supplements like Feverfew (125mg/ day), Riboflavin (400mg/ day), Magnesium (400-600mg/ day) and Co-enzyme Q10 (100mg 3x per day) that have been helpful in preventing headaches for some migraine sufferers. The American Headache Society recommends that patients avoid overuse of medication to control their headaches, (no more than 2 doses per day, 2 days/week) as this can lead to more frequent “rebound” headaches. Do not begin or discontinue any new vitamins or medications without talking to your doctor first, especially if you are nursing or pregnant.
Can Carpal Tunnel Be Prevented?

Carpal Tunnel Syndrome (CTS) is a VERY common condition where the median nerve is compressed or squeezed as it passes through the wrist. One reason that it’s so common is because MANY daily activities require fast, repetitive use of the fingers, hands, and arms, and the friction of the rapidly moving muscle tendons inside the tunnel results in swelling and compression of the nerve. So, can CTS really be prevented?
There are many factors associated with CTS, and some risks can be prevented. For example, some conditions like diabetes, rheumatoid arthritis, and IBS increase the risk of CTS. Therefore, it would be safe to assume those who better manage such conditions would have a lower risk for developing CTS.
Due to the many factors associated with CTS, there is no “one size fits all” when it comes to treatment and prevention of CTS. With that said, here are some VERY effective methods:
1) Ergonomic workstation modifications: Altering the work space (monitor height, keyboard/mouse style, different chair, chair/desk height, etc.) to reduce the number and speed of movements needed to perform commons work tasks.
2) Rest periods: Insert “micro-breaks” into a busy task. Combine breaks with stretching exercises of the wrist/hand/fingers and vary job tasks between fast and slow repetitive types.
3) Exercise: Shake the fingers and hands, lean back in a chair with the arms/shoulders stretched back (“Brugger’s Exercise”), move the neck (chin tucks, rotations, etc.), bend the hand/wrist backwards on a wall or the desk’s edge, self-massage and deep tissue release of the forearm and hand muscles. Do regular aerobic exercise (walking, swimming, biking, etc.) several times each week.
4) Posture: Sit up straight, elbows about 90° on height-adjustable arm rests or comfortably at the sides, forearms parallel to the floor; knees level or slightly lower than the hips, feet flat on the floor or on a footrest or box, if needed. Place typing materials at eye level / avoid prolonged head/neck rotation. Use a wrist rest for the keyboard and mouse, and use a headset when on the phone.
5) Reduce hand tool forces: Choose a tool that allows the wrist to remain neutral. Avoid side to side and flexion/extension wrist positions—especially if they’re prolonged! Tool handles should NOT dig into the palm of the hand or the wrist, and should not have sharp edges. A textured handle can improve grip. Minimize vibration from power tools. Wear shock absorbing gloves. Avoid cold work environments and cold tools.
6) Diet: Cut down on caffeine and smoking. Avoid obesity—a known risk factor of CTS! Consider an anti-inflammatory diet (Paleo, Mediterranean).
7) Splints: A wrist cock-up splint at night prevents prolonged faulty positions and REALLY helps!
This is a partial list of preventative measures that can REALLY help. Doctors of chiropractic treat the WHOLE person and can teach you the right exercises, ways to modify your diet, offer manual therapies and modalities, and help guide you in your self-management of CTS, as this can be a lifelong affliction. A multi-modal treatment approach generally works best!
Trigger points in the pectoralis minor muscle.
The pectoralis minor is a small strap like muscle that is underneath (deep) to the pectoralis major. It originates on the third to fifth rib, near the costal cartilages. It’s insertion is on the coracoid process of the scapula. It acts to draw the scapula forward, downward, and inward at nearly equal angles ( think of rounding or shrugging your shoulders forward). This muscle is very often shortened and tight in people due to the high prevalence of desk jobs. This muscle pulls the shoulder blade forward resulting in the muscles in the back(rhomboid and mid traps) being chronically strained. Trigger points that form in the pec minor primarily refer pain over the anterior chest and shoulder, with spillover down the medial arm. Trigger points in the left side can mimic angina. 
The Bird Dog

Today we are going to look at one of the most effective exercises to protect your lumbar spine from discogenic injury, the bird dog. A great way to work on both posterior chain and rotational stability, the bird dog is safe, effective and simple.
- Get on your hands and knees (four point position) with your knees and hands, hip and shoulders width apart.
- Your back is in neutral position (slightly arched) and your chin must be tucked in.
- Activate your lower abdominals (transversus abdomini) by bringing your belly button inward and by activating your pelvic floor muscles 20 to 30% of maximal contraction.
- Maintain a steady abdominal breathing while you simultaneously lift one leg backwards and the opposite arm overhead keeping your back in neutral position.
- Return to the initial position and repeat with the other leg and arm.
2 sets of 10 reps as part of your regular core/stability routine will have you well on your way to a life-proof low back!
Image and instructions from physiotec.ca
Is Surgery Always Required?
Carpal tunnel syndrome (CTS) is the most common peripheral entrapment neuropathy—that is, it’s the most common place to trap a nerve in the extremities (arms or legs). CTS affects 6-11% of adults in the general population, and it occurs in women more often than men. The cause is often difficult to determine but the most common reasons can include trauma, repetitive maneuvers, certain diseases, pregnancy, being over the age of 50, and obesity.
So, is surgery the only answer? The short answer is NO! In fact, in a recent randomized clinical trial published in the Journal of Pain, researchers observed similar improvements in function when they compared the outcomes of patients who underwent surgery vs. those who received manual therapies (such as those performed several times a day at chiropractic clinics around the world) at both six months and one year later. The improvements included increased strength, function, and decreased hypersensitivity in both the surgical and non-surgical groups. Interestingly, the manual therapy group did BETTER at the one and three month assessments when compared with the surgical group (again, with no difference at six and twelve months)!
The median nerve, the culprit behind CTS, starts in the neck and travels down through the shoulder, elbow, forearm, and finally through the carpal tunnel, which is made up of eight small carpal bones that form the arch of the bridge. Entrapment of the median nerve occurs when the normally tight quarters within the carpal tunnel combine with the inflamed nine sheathed muscle tendons that push the nerve into the floor of the tunnel (a ligament), which results in CTS! The goal of therapy—both surgical and manual therapy—is to reduce the pressure within the tunnel and free up the compression of the median nerve.
Manual therapies focus on joint mobilization and manipulation to reduce joint fixations, muscle release techniques in the forearm and hand, stretching techniques, and at-home exercises that emphasize a similar stretch, the night brace, and management of any underlying contributing factor. These “underlying factors” might include diabetes, hypothyroid, taking birth control pills, weight management, and inflammatory arthritis.

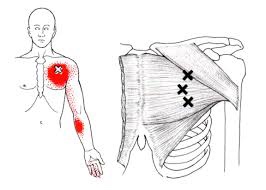
Trigger points in the pectoralis Major muscle.
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
CTS at Night.
For those who have carpal tunnel syndrome (CTS), it’s no surprise that CTS is frequently most expressive during the night, often to the point of interrupting sleep and/or making it difficult to fall back to sleep. So why is that?
The primary reason for nighttime CTS symptoms has to do with the wrist, as it is very difficult to sleep with the wrist held in its “ideal” or least irritating position. In fact, most people favor “curling” the back of the hand under the chin or bending the hand/wrist backwards under the head. When the wrist is bent in either direction, it can increase the pressure inside the wrist, which can generate the various symptoms associated with CTS.
One study evaluated the pressure inside the carpal tunnel while participants slowly moved their wrists. The researchers found many movements didn’t need to exceed 20 degrees before the pressure increased enough within the carpal tunnel to generate symptoms.
Because it doesn’t take a lot of movement to build up excessive pressure in the wrists of those with CTS, many doctors recommend the use of a “cock-up splint” for the non-surgical treatment of CTS in order to help keep the wrist in a neutral position.
Wrist posture is also an important factor during the day. One study looked at typing on a tablet PC, which allowed people to work in non-traditional settings. As screen size reduced, the posture required to type became more limited and accelerated the usual rate of pain onset in the neck, elbows, and wrists.
This study also looked at three different positions used when working on touch-screen devices: desk, lap, and bed. The healthy subjects completed six, 60-minute typing sessions using three virtual keyboard designs: standard, wide, and split. The researchers monitored the position of the wrist, elbow, and neck while the participants typed and followed up each session with questionnaires designed to measure discomfort.
The research team reported that typing in bed required greater wrist extension but resulted in a more natural elbow position than typing at a desk. The angled split keyboard significantly reduced the wrist deviation vs. the standard or wide keyboard designs. All three regions—the neck, elbow, and wrist—exhibited more movements (13% to 38%) towards the end of the one hour sessions, which correlated with a significant increase in pain in every body region investigated. Overall, using a wider keyboard while sitting at a desk was the most tolerable position among study participants.

