Moving is good for your back and muscles, especially if you have back pain. Check out this link for more info!
http://www.theitem.com/stories/exercise-to-help-relieve- your-lower-back-pain,296073
Moving is good for your back and muscles, especially if you have back pain. Check out this link for more info!
http://www.theitem.com/stories/exercise-to-help-relieve- your-lower-back-pain,296073
Fibromyalgia (FM) is a common cause for chronic pain (pain that lasts three or more months) and afflicts 4% of the general population in the United States! FM commonly affects the muscles and soft tissues – not the joints (like arthritis); however, many FM sufferers are mistakenly diagnosed with arthritis, so it may take years before they get an accurate diagnosis. There are NO known accurate diagnostic tests for FM, which is another reason for a delayed diagnosis.
In order to answer the question, “Can fibromyalgia be prevented?” we must first find the cause of FM. There are two types of FM: PRIMARY and SECONDARY. Primary FM occurs for no known reason, while secondary FM can be triggered by a physical event such as a trauma (e.g., car accident), an emotional event or a stressful situation (e.g., loss of a child), and/or a medical event such as a condition like irritable bowel syndrome, rheumatoid arthritis, or systemic lupus erythymatosis (SLE). Any condition that carries chronic or long-lasting symptoms can trigger FM, and some argue that the lack of being able to get into the deep sleep stage may be at the core of triggering FM since sleep disorders are a common finding in FM sufferers!
The “KEY” to managing FM has consistently been and probably always will be EXERCISE and SLEEP. So, if FM is preventable, daily exercise and getting the “right kind” of sleep are very important ways that may reduce the likelihood for developing the condition! Since emotions play a KEY ROLE in the cause and/or effect of FM, applying skills that keep life’s stressors in check is also important. This list can include hobbies like reading a good book, playing and/or listening to music, or meditation. The combination of exercise with mindful meditation using approaches like Tai Chi, Yoga, Qi Gong, and others has had positive impacts on FM patients such as improved balance and stability, reduced pain, enhanced mental clarity, and generally improved quality of life. Managing physical conditions that are associated with FM (such as irritable bowel syndrome, rheumatoid arthritis, or systemic lupus erythymatosis) is also important in managing and/or preventing FM.
Another management strategy of FM is diet. As most patients with FM will agree, certain foods help and others make the FM symptoms worse. In a survey published in the Journal of Clinical Rheumatology, 42% of FM patients reported certain foods exacerbated their symptoms. Of course, each individual case is unique, so keeping a food log or journal can be very helpful to determine dietary “friends” vs. “enemies.” The first step is to eliminate certain foods for four to six weeks, such as dairy and/or gluten. Most patients report a significant improvement in energy (less fatigue) while some report less pain when problem foods are eliminated from their diet. Generally, a diet rich in fruits, vegetables, and lean proteins can have a positive impact on the FM patient. Consider eating multiple small meals vs. two or three large meals during the day, as this can keep blood sugar levels more stable and reduce fatigue.
So back to the question, can fibromyalgia be prevented? Maybe…maybe not. Since the medical community doesn’t know the exact cause, it’s hard to answer this question. However, being proactive and implementing the strategies used to better manage FM may help in preventing it as well!
If you, a friend or family member requires care for Fibromyalgia, we sincerely appreciate the trust and confidence shown by choosing our services!

Becoming healthy and staying healthy is hard, challenging work but worth every second of persistence.

The muscles of the hip provide not only local stability, but also play an important role in spinal and lower extremity functional alignment. (1-4) While weakness in some hip muscles (hip extensors and knee extensors) is well tolerated, weakness or imbalance in others can have a profound effect on gait and biomechanical function throughout the lower half of the body. (5) Weakness of the hip abductors, particularly those that assist with external rotation, has the most significant impact on hip and lower extremity stability. (5,6)

The gluteus medius is the principal hip abductor. When the hip is flexed, the muscle also assists the six deep hip external rotators (piriformis, gemelli, obturators, and quadratus femoris). The gluteus medius originates on the ilium just inferior to the iliac crest and inserts on the lateral and superior aspects of the greater trochanter. While the principal declared action of the gluteus medius is hip abduction, clinicians will appreciate its more valuable contribution as a dynamic stabilizer of the hip and pelvis- particularly during single leg stance activities like walking, running, and squatting. The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance. The remainder comes predominantly from 2 muscles that insert onto the iliotibial band: the tensor fascia lata and upper gluteus maximus. Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity. (6)
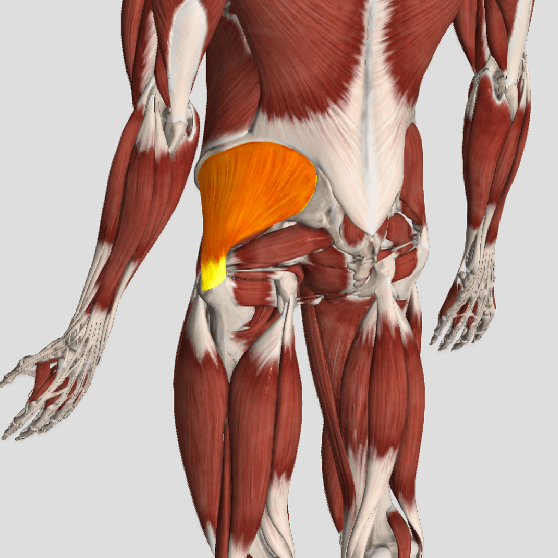
Incompetent hip abductors and/or external rotators allows for excessive adduction and internal rotation of the thigh during single leg stance activities. This leads to a cascade of biomechanical problems, including pelvic drop, excessive hip adduction, excessive femoral internal rotation, valgus knee stress, and internal tibial rotation. (1,7-12)

https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2517920#ioi160017r18
Some very interesting findings in this study. Over the course of two years participants who were part of the fasting group showed a weight loss of 10% on average as well as improved perceptions of quality of life, energy, sleep quality and libido.
Is fasting right for you? That depends and it is an idea that you and your health care professional should discuss as what works for some may not be right for you.
By Bryan Cobb, Advanced Remedial Massage Therapist

What is a Trigger Point?
Trigger Points (TP’s) are defined as a “hyper-irritable spot within a taut band of skeletal muscle. The spot is painful on compression and can evoke characteristic referred pain and autonomic phenomena.”1
Put into plain language, a TP is a painful knot in muscle tissue that can refer pain to other areas of the body. You have probably felt the characteristic achy pain and stiffness that TP’s produce, at some time in your life.
TP’s were first brought to the attention of the medical world by Dr. Janet G. Travell. Dr. Travell, physician to President John F. Kennedy, is the acknowledged Mother of Myofascial Trigger Points. In fact, “Trigger Point massage, the most effective modality used by massage therapists for the relief of pain, is based almost entirely on Dr. Travell’s insights.”2 Dr. Travell’s partner in her research was Dr. David G. Simons, a research scientist and aerospace physician.
Trigger Points are very common. In fact, Travell and Simons state that TP’s are responsible for, or associated with, 75% of pain complaints or conditions.1 With this kind of prevalence, it’s no wonder that TP’s are often referred to as the “scourge of mankind”.
Trigger Points can produce a wide variety of pain complaints. Some of the most common are migraine headaches, back pain, and pain and tingling into the extremities. They are usually responsible for most cases of achy deep pain that is hard to localize.
A TP will refer pain in a predictable pattern, based on its location in a given muscle. Also, since these spots are bundles of contracted muscle fibres, they can cause stiffness and a decreased range of motion. Chronic conditions with many TP’s can also cause general fatigue and malaise, as well as muscle weakness.
Trigger Points are remarkably easy to get, but the most common causes are
TP’s (black X) can refer pain to other areas (red)
Sudden overload of a muscle
Once in place, a TP can remain there for the remainder of your life unless an intervention takes place.
Trigger Points Not Well Known
With thousands of people dealing with chronic pain, and with TP’s being responsible for — or associated with — a high percentage of chronic pain, it is very disappointing to find that a large portion of doctors and other health care practitioners don’t know about TP’s and their symptoms.
Scientific research on TP’s dates back to the 1700’s. There are numerous medical texts and papers written on the subject.
But, it still has been largely overlooked by the health care field. This has led to needless frustration and suffering, as well as thousands of lost work hours and a poorer quality of life.
How Are Trigger Points Treated?
As nasty and troublesome as TP’s are, the treatment for them is surely straight-forward. A skilled practitioner will assess the individual’s pain complaint to determine the most likely location of the TP’s and then apply one of several therapeutic modalities, the most effective of which is a massage technique called “ischemic compression”.
Basically, the therapist will apply a firm, steady pressure to the TP, strong enough to reproduce the symptoms. The pressure will remain until the tissue softens and then the pressure will increase appropriately until the next barrier is felt. This pressure is continued until the referral pain has subsided and the TP is released. (Note: a full release of TP’s could take several sessions.)
Other effective modalities include dry needling (needle placed into the belly of the TP) or wet needling (injection into the TP). The use of moist heat and stretching prove effective, as well. The best practitioners for TP release are Massage Therapists, Physiotherapists, and Athletic Therapists. An educated individual can also apply ischemic compression to themselves, but should start out seeing one of the above therapists to become familiar with the modality and how to apply pressure safely.
1 Simons, D.G., Travell, D.G., & Simons, L.S. Travell and Simons’Myofascial Pain and Dysfunction: the Trigger Point Manual.
Vol. 1. 2nd ed. Lippincott, Williams, and Wilkins, 1999.

Patellofemoral pain syndrome (PFPS), also called “Runners Knee”, describes the symptom complex of knee discomfort, swelling, or crepitus that results from excessive or imbalanced forces acting on the joint. It is the most common cause of knee pain in the general population, affecting an estimated 25% of adults.
PFPS is most commonly related to lateral tracking of the patella. The patella has a natural tendency to migrate laterally due to the pull of the quadriceps and the slight natural valgus of the lower extremity. A new study in the Journal of Sports Medicine (1) provides additional confirmation that when managing patellofemoral pain syndrome, clinicians must address two critical yet often overlooked issues.
This study concludes that PFPS and dynamic knee valgus do not arise primarily from knee dysfunction, rather from hip abductor/ external rotator weakness and/or foot hyperpronation.
“The most effective intervention programs included exercises targeting the hip external rotator and abductor muscles and knee extensor muscles.” and “PFPS patients with foot abnormalities, such as those with increased rearfoot eversion or pes pronatus, may benefit the most from foot orthotics.”
Since gluteus medius and VMO weakness are key factors in the development of PFPS, strengthening exercises that target those muscles prove most effective. Stabilization exercises may include pillow push (push the back of your knee into a pillow for 5-6 seconds), supine heel slide, terminal knee (short-arc) extension, clam, glut bridge, semi-stiff deadlift, posterior lunge, and monster walk.
Myofascial release and stretching should be directed at hypertonic muscles, including the TFL, gastroc, soleus, hamstring, piriformis, hip rotators, and psoas. Myofascial release or IASTM may be appropriate for tightness in the iliotibial band, vastus lateralis, posterior hip capsule, and lateral knee retinaculum.
Manipulation may be necessary for restrictions in the lumbosacral and lower extremity joints. Hypermobility is common in the ipsilateral SI joint with restrictions present contralaterally. Evidence has shown that patellar tracking braces, i.e. BioSkin® or PatellaPro®, may lead to better outcomes.
Lifestyle modification may be necessary to reduce pain-provoking endeavors, especially running, jumping and other activities that induce a valgus stress. Athletes should avoid allowing their knee to cross in front of their toes while squatting. Arch supports or custom orthotics may be necessary to correct hyperpronation. Runners should avoid cross-over gaits and change shoes every 250 to 500 miles.
.
.
.
.
.
.
.
#pain
#kneepain
#chiropractic
#fitness
#sports
#wellness
#fitness
#healthyliving
#healthychoices
#Winnipeg
References
1. Petersen W, Rembitzki I, Liebau C. Patellofemoral pain in athletes. Open Access Journal of Sports Medicine. 2017;8:143-15