The pectoralis minor is a small strap like muscle that is underneath (deep) to the pectoralis major. It originates on the third to fifth rib, near the costal cartilages. It’s insertion is on the coracoid process of the scapula. It acts to draw the scapula forward, downward, and inward at nearly equal angles ( think of rounding or shrugging your shoulders forward). This muscle is very often shortened and tight in people due to the high prevalence of desk jobs. This muscle pulls the shoulder blade forward resulting in the muscles in the back(rhomboid and mid traps) being chronically strained. Trigger points that form in the pec minor primarily refer pain over the anterior chest and shoulder, with spillover down the medial arm. Trigger points in the left side can mimic angina. 
Chronic Pain
Is Surgery Always Required?
Carpal tunnel syndrome (CTS) is the most common peripheral entrapment neuropathy—that is, it’s the most common place to trap a nerve in the extremities (arms or legs). CTS affects 6-11% of adults in the general population, and it occurs in women more often than men. The cause is often difficult to determine but the most common reasons can include trauma, repetitive maneuvers, certain diseases, pregnancy, being over the age of 50, and obesity.
So, is surgery the only answer? The short answer is NO! In fact, in a recent randomized clinical trial published in the Journal of Pain, researchers observed similar improvements in function when they compared the outcomes of patients who underwent surgery vs. those who received manual therapies (such as those performed several times a day at chiropractic clinics around the world) at both six months and one year later. The improvements included increased strength, function, and decreased hypersensitivity in both the surgical and non-surgical groups. Interestingly, the manual therapy group did BETTER at the one and three month assessments when compared with the surgical group (again, with no difference at six and twelve months)!
The median nerve, the culprit behind CTS, starts in the neck and travels down through the shoulder, elbow, forearm, and finally through the carpal tunnel, which is made up of eight small carpal bones that form the arch of the bridge. Entrapment of the median nerve occurs when the normally tight quarters within the carpal tunnel combine with the inflamed nine sheathed muscle tendons that push the nerve into the floor of the tunnel (a ligament), which results in CTS! The goal of therapy—both surgical and manual therapy—is to reduce the pressure within the tunnel and free up the compression of the median nerve.
Manual therapies focus on joint mobilization and manipulation to reduce joint fixations, muscle release techniques in the forearm and hand, stretching techniques, and at-home exercises that emphasize a similar stretch, the night brace, and management of any underlying contributing factor. These “underlying factors” might include diabetes, hypothyroid, taking birth control pills, weight management, and inflammatory arthritis.

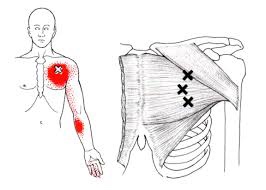
Trigger points in the pectoralis Major muscle.
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Why am I so dizzy after my whiplash?

Whiplash, or better termed “Whiplash Associated Disorders” (WAD), is a condition that carries multiple signs and symptoms ranging from neck pain and stiffness to headache, confusion, ringing in the ears, and more. But can WAD cause dizziness? Let’s take a look!
Dizziness is a general term that is used rather loosely by the general population. We’ve all experienced dizziness from time-to-time that is considered “normal,” such as standing up too quickly or while experiencing a rough flight.
Often, dizziness and problems with balance go hand in hand. There are three main organs that control our balance: 1) the vestibular system (the inner ear); 2) the cerebellum (lies in the back of the head); and, 3) the dorsal columns (located in the back part of the spinal cord). In this article, we will primarily focus on the inner ear because, of the three, it’s unique for causing dizziness. Our vision also plays an important role in maintaining balance, as we tend to lose our balance much faster when we close our eyes.
It’s appropriate to first discuss the transient, usually short episode of “normal” lightheadedness associated with rising quickly. This is typically caused by a momentary drop in blood pressure, and hence, oxygen simply doesn’t reach the brain quick enough when moving from sitting to standing. Again, this is normal and termed “orthostatic hypotension” (OH).
However, OH can be exaggerated by colds, the flu, allergy flair-ups, when hyperventilating, or at times of increased stress or anxiety. OH is also associated with the use of tobacco, alcohol, and/or some medications. Bleeding can represent a more serious cause of OH such as with bleeding ulcers or some types of colitis, and less seriously, with menstruation.
The term BPPV or benign paroxysmal positional vertigo, has to do with the inner ear where our semicircular canals are located. The canals lie in three planes and give us a 3D, 360º perspective about where we are in space. The fluid flowing through these canals bends little hair-like projections, which are connected to sensory nerves that tell the brain about our spatial position. If the function of these canals is disturbed, it can mix-up the messages the brain receives, thus resulting in dizziness. Exercises are available on the Internet that can help with BPPV (look for Epley’s and Brandt-Daroff exercises).
DANGEROUS causes of dizziness include: HEART – fainting (passing out) accompanied by chest pain, shortness of breath, nausea, pain or pressure in the back, neck, jaw, upper belly, or in one or both arms, sudden weakness, and/or a fast or irregular heartbeat.
STROKE – sudden numbness, paralysis, or weakness in the face, arm, or leg, especially if only on one side of the body; drooling, slurred speech, short “black outs,” sudden visual changes, confusion/difficulty speaking, and/or a sudden and severe, “out of the ordinary” headache. CALL 911 (or the number for emergency services if you’re outside the Canada) if you suspect you may be having a heart attack or stroke!
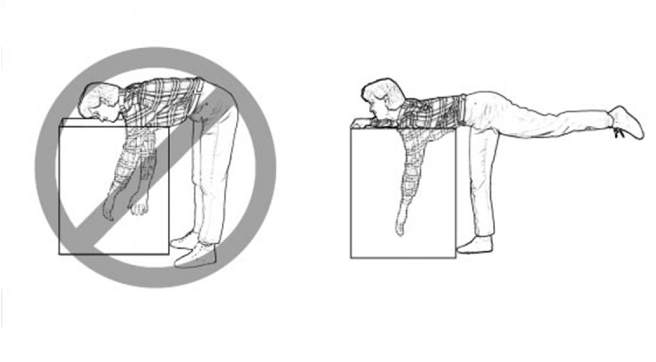
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
CTS at Night.
For those who have carpal tunnel syndrome (CTS), it’s no surprise that CTS is frequently most expressive during the night, often to the point of interrupting sleep and/or making it difficult to fall back to sleep. So why is that?
The primary reason for nighttime CTS symptoms has to do with the wrist, as it is very difficult to sleep with the wrist held in its “ideal” or least irritating position. In fact, most people favor “curling” the back of the hand under the chin or bending the hand/wrist backwards under the head. When the wrist is bent in either direction, it can increase the pressure inside the wrist, which can generate the various symptoms associated with CTS.
One study evaluated the pressure inside the carpal tunnel while participants slowly moved their wrists. The researchers found many movements didn’t need to exceed 20 degrees before the pressure increased enough within the carpal tunnel to generate symptoms.
Because it doesn’t take a lot of movement to build up excessive pressure in the wrists of those with CTS, many doctors recommend the use of a “cock-up splint” for the non-surgical treatment of CTS in order to help keep the wrist in a neutral position.
Wrist posture is also an important factor during the day. One study looked at typing on a tablet PC, which allowed people to work in non-traditional settings. As screen size reduced, the posture required to type became more limited and accelerated the usual rate of pain onset in the neck, elbows, and wrists.
This study also looked at three different positions used when working on touch-screen devices: desk, lap, and bed. The healthy subjects completed six, 60-minute typing sessions using three virtual keyboard designs: standard, wide, and split. The researchers monitored the position of the wrist, elbow, and neck while the participants typed and followed up each session with questionnaires designed to measure discomfort.
The research team reported that typing in bed required greater wrist extension but resulted in a more natural elbow position than typing at a desk. The angled split keyboard significantly reduced the wrist deviation vs. the standard or wide keyboard designs. All three regions—the neck, elbow, and wrist—exhibited more movements (13% to 38%) towards the end of the one hour sessions, which correlated with a significant increase in pain in every body region investigated. Overall, using a wider keyboard while sitting at a desk was the most tolerable position among study participants.

Trigger points in the rhomboid muscles.
This is another common muscle to get trigger points. It originates on the spinous processes of the T2-T5 vertebrae. It inserts on the medial border of the scapula. It’s main actions are to adduct the scapula pulling it back toward the spine, and to rotate the glenohumeral joint downward. This muscle also prevents wining of the scapula. This muscle is often overloaded by a sitting posture where the shoulders are rolled forward such as when using a computer. The Rhomboids are often weak and under trained in people. Trigger points in this muscle cause pain and ache in the upper back between the shoulder blade. Strength trading for this muscle is necessary to help prevent postural overload. 
Trigger points in the trapezius muscle.
The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
My back hurts, why look at my feet?

Improperly supported feet can affect the alignment of all of the structures above. To improve your overall comfort:
✓ Choose shoes with good arch support.
✓ Avoid going barefoot or wearing shoes that lack support (i.e. flip-flops). The following brands of sandals provide better than average arch support: Naot, Fit Flops, Orthoheels, Abeo, Vionic and Yellow box.
✓ Avoid high-heeled shoes or boots (keep heels to a maximum of 1½ inches, especially if you are going to be doing a lot of walking).
✓ “Cross-trainer” athletic shoes tend to provide the best all around support and shock absorption for daily activities.
✓ Patients with fallen arches should consider adding arch supports or orthotics.
✓ Repair or replace shoes with worn soles or heels.
Lifting Mechanics Made Simple

Here are some tips to help you lift safely:
✓ Avoid lifting or flexing before you’ve had the chance to warm up your muscles (especially when you first awaken or after sitting or stooping for a period of time).
✓ To lift, stand close directly facing object with your feet shoulder width apart.
✓ Squat down by bending with your knees, not your back. Imagine a fluorescent light tube strapped to your head and hips when bending. Don’t “break” the tube with improper movements. Tuck your chin to help keep your spine aligned.
✓ Slowly lift by thrusting your hips forward while straightening your legs.
✓ Keep the object close to your body, within your powerzone” between your hips and chest. Do not twist your body, if you must turn while carrying an object, reposition your feet, not your torso.
An alternative lifting technique for smaller objects is the golfers lift. Swing one leg directly behind you. Keep your back straight while your body leans forward. Placing one hand on your thigh or a sturdy object may help.