The gluteus Maximus is the buttock muscle. It originates on the gluteal surface of the ilium, lumbar fascia, sacrum and sacrotuberous ligament. It inserts on the gluteal tuberosity of the femur and the iliotibial tract. Extension and lateral rotation of the hip are it’s main actions. This muscle is heavily involved in activities like ice skating and is a common area to develops trigger points. When trigger points do develop they can refer pain in a crescent pattern from the gluteal fold to the sacrum. Trigger points can also refer pain deep into the buttock itself making it feel like other deeper muscles are involved. These symptoms can sometimes be mistaken for s.i. Joint problems. 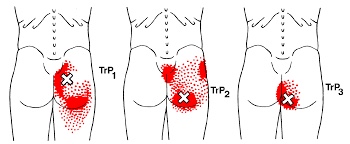
Meditation goes mainstream!

With growing evidence that meditation has significant health benefits, a 2016 study by a team of researchers from the United States, Spain, and France sought to explain how and why meditation actually works.
The study investigated the difference between “mindful meditation” in a group of experienced meditators vs. “quiet non-meditative activity” in a group of untrained control subjects. After eight hours of mindfulness practice, the meditation group showed a range of genetic and molecular differences, which in turn correlated with faster physical recovery from a stressful situation.
According to researchers, this is the first time a study has documented a rapid alteration in gene expression within meditating subjects. Interestingly, the researchers observed these changes in the SAME genes that anti-inflammatory and pain-killing drugs target! Thus, they speculate that mindful-based training may benefit patients with inflammatory conditions! This and prior studies have prompted the American Heart Association to endorse meditation as an effective cardiac preventative intervention.
Meditation has been found to be helpful for many conditions including stress management, lowering high blood pressure, heart disease, and depression. You can incorporate meditation into your life with three simple meditation exercises! The initial advice is “…go slow and be compassionate and gentle with yourself.” Your mind will try to wander (called our “default mode”) which consumes about half of our day, so try to focus (called “focus mode”)!
1) WALKING MEDITATION: At a slow to medium pace, focus on your feet. Notice how your heel hits the ground and then feel the roll of your foot followed by the big toe pushing off prior to the swing phase. Feel for stones under the foot and other interesting sensations. If your mind starts to wander (default mode), gently bring your attention back to your foot (focus mode). You WILL get better with practice, and you’ll soon find it much easier to “focus” during stressful situations!
2) NOVEL EXPERIENCES: It’s much easier to lose focus on the people you see everyday vs. those seen only one time a month. The next time you arrive home from work, pretend you haven’t seen your spouse/friend in 30 days. Give them your undivided attention. Then, try this on co-workers and other people you see every day. Believe me, they WILL notice a difference!
3) GRATITUDE EXERCISES: When you’re not in their presence, focus on a person’s face and send them a “silent gratitude” for being in your life. Try this on family members, friends, co-workers, and others!

SI Joint Dysfunction. Nothing FUN about it.
Your sacroiliac joint is the mechanical link on each side of your hip that connects your legs to the rest of your body. The joint has a limited but very important degree of mobility. Symptoms develop when one or both of the joints loses normal motion. When a joint becomes “restricted”, a self-perpetuating cycle of discomfort follows. Restriction causes the muscles to become overworked, leading to tightness, compression, inflammation, pain and more restriction.
 Sacroiliac problems can happen as a result of repetitive strenuous activity or trauma- like a fall onto the buttocks. Other causes of sacroiliac joint problems include, poor posture, having one leg slightly longer than another, having an altered gait, having flat feet or scoliosis, or having pain somewhere else in your legs. Pregnancy is a common trigger for sacroiliac joint problems due to weight gain, gait changes and postural stress.
Sacroiliac problems can happen as a result of repetitive strenuous activity or trauma- like a fall onto the buttocks. Other causes of sacroiliac joint problems include, poor posture, having one leg slightly longer than another, having an altered gait, having flat feet or scoliosis, or having pain somewhere else in your legs. Pregnancy is a common trigger for sacroiliac joint problems due to weight gain, gait changes and postural stress.
Sacroiliac joint problems often begin as a focal discomfort in your back just below the belt line, slightly to one side of center. Your pain can travel into your buttock or thigh. Symptoms are often worse by standing on the affected side. The pain may become more apparent when you change positions- like exiting a chair, car or bed, or during long car rides. The pain is often relieved by lying down.
To assist with your recovery, you should avoid any activity that provokes pain, like standing on the affected leg or prolonged sitting.
The Medial Ankle Sprain. “The Other Sprain”.
“Ligaments” are made up of many individual fibers running parallel to each other and bundled to form a strong fibrous band. These fibrous bands hold your bones together. Just like a rope, when a ligament is stretched too far, it begins to fray or tear. “Sprain” is the term used to describe this tearing of ligament fibers.
Sprains are graded by the severity of damage to the ligament fibers. A Grade 1 sprain means the ligament has been painfully stretched, but no fibers have been torn. A Grade 2 sprain means some, but not all, of the ligaments’ fibers have been torn. A Grade 3 sprain means all of the ligaments’ fibers have been torn, and the ligament no longer has the ability to protect the joint.


Ankle sprains are the most common soft-tissue injury and will affect up to 20% of active people at some point in their life. Most ankle sprains occur because you have “rolled your ankle”. Sprains like yours, involving the inside of your ankle (medial) are much less common than injuries to the outer side. Medial ankle sprains are often accompanied by other injuries like “high ankle sprains” or fractures.
Ankle sprains cause pain and swelling over the inside of your ankle. Walking may be difficult, and bruising is common. Be sure to tell your doctor if you experience numbness, tingling, or a dramatic cold sensation in your foot, as this may indicate more significant injury.
Ankle sprains can be successfully managed but will require some work on your part. You can help reduce swelling by elevating your ankle by lying or sitting with your foot elevated or by using an ACE wrap for compression. Applying ice or ice massage for 10 minutes each hour may help relieve swelling. Depending upon the severity of your sprain, you may need to wear an ankle brace to help protect you from further injury. If walking is painful, crutches may be necessary.
Initially, a period of rest may be necessary in order to help you heal. Mild Grade 1 sprains may allow return to sport in a couple of days, while more severe injuries may take six weeks or longer to recover.
Turf Toe? What Is That?
“Turf toe” means that the strong fibrous ligaments connecting your big toe to your foot have been stretched too far and have been “sprained.” This most commonly happens when your big toe is extended forcibly toward the top of your foot. This may happen abruptly from a fall or when something lands on the back of your calf while your toes are touching the ground. Turf toe commonly occurs from jamming your big toe into a hard surface. Occasionally, the injury happens over a long period of time from repetitive stress- like pushing off of the big toe each time you run or jump.

The term “turf toe” was coined because this injury became more common in athletes with the implementation of artificial turf fields. Turf toe injuries rank third after knee and ankle injuries among the most common cause for lost playing time in athletes.
A turf toe injury causes pain and swelling at the base of your big toe. You will notice your pain probably increases when your toe is straightened or bent backward toward the top of your foot. Sometimes you may notice bruising shortly after the injury. Gout, a type of arthritis that is more common in men, can sometimes act like turf toe. Be sure to tell your doctor if you or someone in your family has a history of gout.
Early treatment is focused on keeping your toe from moving too much. Depending upon the severity of the injury, turf toe usually requires a period of rest for proper healing. When directed, you may begin non-weight bearing activities, such as stationary cycling or swimming. You should take a close look at your shoes before returning to play. Wearing excessively flexible shoes on a turf field increases your chance of injury. Consider a stiff-soled shoe or hard carbon fiber insert during initial healing. When you are able to run and change directions without pain or loss of mobility, you will likely be allowed to return to play. Be sure to ice your toe for 10-15 minutes following any activity while your injury is healing.
Trigger points in the supraspinatus
The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.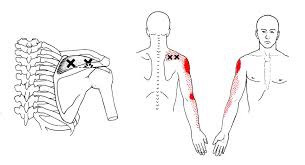
Can Chiro help me?

Chiropractic is the most widely accepted and most frequently used type of “alternative” healthcare in the United States. This is largely due to the fact that it works, and because of that, there has been a steady increase in acceptance by the public, third-party payers, and the Federal government. Since the mid-1990s, a number of outside (non-chiropractic) observers have suggested that chiropractic has now entered mainstream healthcare.
One can position chiropractic as being BOTH alternative and mainstream. It is “alternative” since it approaches healthcare from an entirely different direction compared to the primary care medical profession. Chiropractic is non-surgical and promotes diet and nutritional approaches vs. drugs and surgery. Chiropractic is also arguably “mainstream” as it has evolved into a strongly utilized form of primary care through popular acceptance and utilization by the public.
So, what role does chiropractic play in today’s health delivery system? This question is still being debated, but there appears to be three camps: 1) Specialist—limited to musculoskeletal (MSK) complaints on an interdisciplinary primary healthcare team; 2) Primary healthcare “gatekeepers” that focus on ambulatory MSK complaints; 3) Generalist primary healthcare provider of “alternative or complementary” medicine that manage and/or co-manage both MSK AND non-MSK conditions.
Looking at this from the patient or “consumer” perspective, chiropractic already plays an important role in the healthcare delivery for many patients. In 1993, a report claimed 7% of American adults had received chiropractic care during the prior year. According to a 2015 Gallup poll (that included 5,442 adults, aged 18+, surveyed between 2/16/15 and 5/6/15) entitled, Majority in U.S. Say Chiropractic Works for Neck, Back Pain, “Chiropractic care has a positive reputation among many US adults for effective treatment of neck and back pain, with about six in 10 adults either strongly agreeing (23%) or agreeing somewhat (38%) that chiropractors are effective at treating these types of pain.”
The “highlights” from this Gallup poll include: 1) Two-thirds say chiropractic is effective for neck and back pain. 2) Many adults say chiropractors think of the patient’s best interest. 3) More than 33 million adults in the United States (US) saw a chiropractor in the twelve months before the survey was conducted. That means roughly 14% of U.S. adults saw a chiropractor in the 12 months prior to the survey (vs. 7% in 1993). An additional 12% who responded to the Gallup pollsters saw a chiropractor in the last five years but not in the last 12 months. Overall, 51% of those polled had previously seen a chiropractor.
Whether or not you have personally utilized chiropractic, the educational process, licensing requirements, public interest, third-party payer systems, and interprofessional cooperation ALL support firm ground for which you can comfortably and confidently seek chiropractic care for your complaints.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care, we would be honored to render our services.

My ankle hurts…….
The posterior tibialis muscle begins deep in your calf. The muscle is connected to the arch of your foot by a tendon that runs along the inside of your ankle, just behind the large bump called the medial malleolus. When you walk, the posterior tibialis muscle lifts the arch of your foot. 
Posterior tibial tendon dysfunction is one of the most common foot and ankle problems. The tendon may be damaged from an acute injury, like an accident or fall. More commonly, problems arise from overuse or repeated strain. Ongoing irritation slowly damages the tendon’s fibers and eventually leads to weakening and degeneration. This decreases the tendon’s ability to support your foot when you walk. As the tendon becomes less effective, the arch of your foot is allowed to collapse, which further increases the strain on the muscle and tendon.
The condition is often triggered from overuse and/or training on excessively hard surfaces. Other factors that can contribute to posterior tibial tendon dysfunction include: obesity, diabetes, hypertension, prior surgery or steroid injections.
Symptoms include pain or swelling along the course of the tendon, particularly behind your inner ankle bone. Symptoms often begin following an increase in training intensity or duration. Standing, walking, or running will likely increase your discomfort. Your pain may be aggravated by spending prolonged periods of time on your feet, especially, when standing tiptoe and walking stairs or uneven surfaces.
Early diagnosis and treatment is important to slow progression of the disorder. You may need to temporarily limit weight-bearing activity to allow your tendon to heal. Using a stationary cycle, elliptical machine, or swimming can be good alternatives to walking and running. Your doctor will likely prescribe arch supports or orthotics to help support your foot. You will be given exercises to strengthen the posterior tibialis muscle. These exercises should be performed while wearing shoes with good arch supports. In certain instances, a walking cast or boot may be needed to temporarily protect your foot.
