Moving is good for your back and muscles, especially if you have back pain. Check out this link for more info!
http://www.theitem.com/stories/exercise-to-help-relieve- your-lower-back-pain,296073
Moving is good for your back and muscles, especially if you have back pain. Check out this link for more info!
http://www.theitem.com/stories/exercise-to-help-relieve- your-lower-back-pain,296073
Fibromyalgia (FM) is a common cause for chronic pain (pain that lasts three or more months) and afflicts 4% of the general population in the United States! FM commonly affects the muscles and soft tissues – not the joints (like arthritis); however, many FM sufferers are mistakenly diagnosed with arthritis, so it may take years before they get an accurate diagnosis. There are NO known accurate diagnostic tests for FM, which is another reason for a delayed diagnosis.
In order to answer the question, “Can fibromyalgia be prevented?” we must first find the cause of FM. There are two types of FM: PRIMARY and SECONDARY. Primary FM occurs for no known reason, while secondary FM can be triggered by a physical event such as a trauma (e.g., car accident), an emotional event or a stressful situation (e.g., loss of a child), and/or a medical event such as a condition like irritable bowel syndrome, rheumatoid arthritis, or systemic lupus erythymatosis (SLE). Any condition that carries chronic or long-lasting symptoms can trigger FM, and some argue that the lack of being able to get into the deep sleep stage may be at the core of triggering FM since sleep disorders are a common finding in FM sufferers!
The “KEY” to managing FM has consistently been and probably always will be EXERCISE and SLEEP. So, if FM is preventable, daily exercise and getting the “right kind” of sleep are very important ways that may reduce the likelihood for developing the condition! Since emotions play a KEY ROLE in the cause and/or effect of FM, applying skills that keep life’s stressors in check is also important. This list can include hobbies like reading a good book, playing and/or listening to music, or meditation. The combination of exercise with mindful meditation using approaches like Tai Chi, Yoga, Qi Gong, and others has had positive impacts on FM patients such as improved balance and stability, reduced pain, enhanced mental clarity, and generally improved quality of life. Managing physical conditions that are associated with FM (such as irritable bowel syndrome, rheumatoid arthritis, or systemic lupus erythymatosis) is also important in managing and/or preventing FM.
Another management strategy of FM is diet. As most patients with FM will agree, certain foods help and others make the FM symptoms worse. In a survey published in the Journal of Clinical Rheumatology, 42% of FM patients reported certain foods exacerbated their symptoms. Of course, each individual case is unique, so keeping a food log or journal can be very helpful to determine dietary “friends” vs. “enemies.” The first step is to eliminate certain foods for four to six weeks, such as dairy and/or gluten. Most patients report a significant improvement in energy (less fatigue) while some report less pain when problem foods are eliminated from their diet. Generally, a diet rich in fruits, vegetables, and lean proteins can have a positive impact on the FM patient. Consider eating multiple small meals vs. two or three large meals during the day, as this can keep blood sugar levels more stable and reduce fatigue.
So back to the question, can fibromyalgia be prevented? Maybe…maybe not. Since the medical community doesn’t know the exact cause, it’s hard to answer this question. However, being proactive and implementing the strategies used to better manage FM may help in preventing it as well!
If you, a friend or family member requires care for Fibromyalgia, we sincerely appreciate the trust and confidence shown by choosing our services!

Whiplash Associated Disorders (WAD) is the appropriate terminology to use when addressing the myriad of symptoms that can occur as a result of a motor vehicle collision (MVC). In a recent publication in The Physician and Sports Medicine (Volume 43, Issue 3, 2015; 7/3/15 online:1-11), the article “The role of the cervical spine in post-concussive syndrome” takes a look at the neck when it’s injured in a car accident and how this relates to concussion.
It’s estimated about 3.8 million concussion injuries, also referred to as “mild traumatic brain injury” (mTBI), occur each year in the United States. Ironically, it’s one of the least understood injuries in the sports medicine and neuroscience communities. The GOOD NEWS is that concussion symptoms resolve within 7-10 days in the majority of cases; unfortunately, this isn’t the case with 10-15% of patients. Symptoms can last weeks, months, or even years in this group for which the term “post-concussive syndrome” (PCS) is used (defined as three or more symptoms lasting for four weeks as defined by the ICD-10) or three months following a minor head injury (as defined by the Diagnostic and Statistical Manual of Mental Disorders).
There have been significant advances in understanding what takes place in the acute phase of mTBI, but unfortunately, there is no clear physiological explanation for the chronic phase. Studies show the range of force to the head needed to cause concussion is between 60-160g (“g” = gravity) with 96.1g representing the highest predictive value in a football injury, whereas as little as 4.5g of neck acceleration can cause mild strain injury to the neck. In spite of this difference, the signs and symptoms reported by those injured in low-speed MVCs vs. football collisions are strikingly similar!
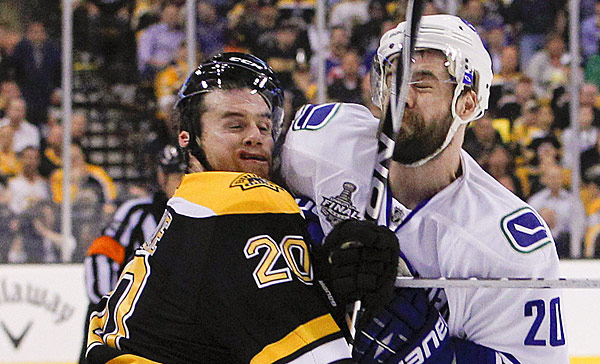
Research shows if an individual sustains an injury where the head is accelerated between 60-160g, it is HIGHLY likely that the tissues of the cervical spine (neck) have also reached their injury threshold of 4.5g. In a study that looked at hockey players, those who sustained a concussion also had WAD / neck injuries indicating that these injuries occur concurrently. Injuries to the neck in WAD include the same symptoms that occur in concussion including headache, dizziness/balance loss, nausea, visual and auditory problems, and cognitive dysfunction, just to name a few.
The paper concludes with five cases of PCS that responded well to a combination of active exercise/rehabilitation AND passive manual therapy (cervical spine manipulation). The favourable outcome supports the concept that the neck injury portion of WAD is a very important aspect to consider when treating patients with PCS!
This “link” between neck injury and concussion explains why chiropractic care is essential in the treatment of the concussion patient! This is especially true when the symptoms of concussion persist longer than one month!
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honoured to render our services.

Becoming healthy and staying healthy is hard, challenging work but worth every second of persistence.

Thank you to all of our patients. It is always a pleasure to serve you and we appreciate your trust and confidence when you refer others to our clinic.

Be careful out there on the roads tonight! Kids are everywhere!