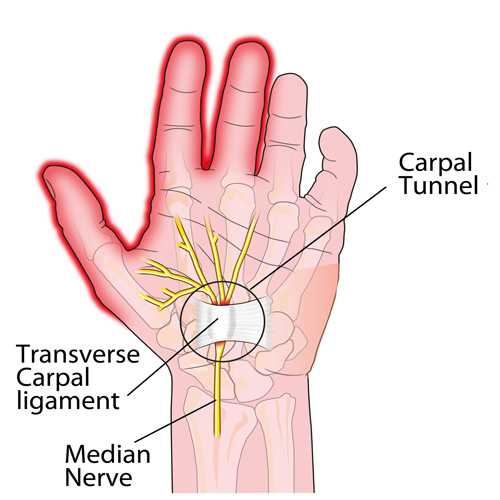
Here it is: carpal tunnel syndrome (CTS) in a nutshell!
Define what makes you your best self. Define what makes you happy, healthy and well and stop at nothing to get there.
In 2015, two million Americans had a substance abuse disorder involving prescription pain relievers; with more than 20,000 overdose deaths related to these drugs. In the past decade, death rates and substance use rates quadrupled in parallel to sales of prescription pain relievers.
Chronic LBP is a primary generator for opioid prescriptions. This year, both JAMA and Annals of Internal Medicine have published and supported new clinical practice guidelines that recommend prescribing spinal manipulation over medication for LBP patients.
“For acute, subacute, or chronic low back pain, physicians and patients initially utilize spinal manipulation and delay pharmacologic management.”
Research shows that low back pain patients who undergo chiropractic care have improved outcomes with lower rates of opioid use, surgery, and overall healthcare costs.
Not surprisingly, various governing bodies, including the FDA, CDC, and 37 State Attorney General’s, have concurred that physicians and healthcare decision makers should consider non- pharmacologic therapy for LBP patients. In fact, the 2018 Joint Commission guidelines mandate that hospitals include conservative options for chronic musculoskeletal pain management, specifically naming chiropractic as a potential option.
Chiropractic care is not a replacement for traditional medical treatment of LBP, rather a complementary tool to integrate within your current management paradigm. We hope that you will continue to consider our office for those cases that may be favorably served by conservative manual therapy. We are grateful for your confidence and will work hard to maintain your trust.



Some things to consider if you’re suffering from back pain.
Reasons you’re probably suffering from back pain (besides sitting all day)