The trapezius muscle is a large diamond shaped muscle in your back and neck. It originates on the nuchal ligament and the spinous processes of c6-t12. It inserts on the scapular spine, acromion process, and the distal clavicle. It’s upper fibres act to elevate the shoulder and rotate the glenoid fossa upward. The lower fibres assist this motion. The middle fibres strongly adduct the scapula. This is the most common muscle in the human body to get trigger points. Trigger points in the lateral upper edge refer pain into the lateral neck and temples. Points in the mid and lower parts of the muscle refer pain into the posterior neck and shoulders. Trigger points in this muscle are a common cause of headaches.
Winnipeg Chiropractor
Elbow pain and trigger points.
Did you know that tennis elbow and golfers elbow pain can be caused by trigger points? Points located in the forearm flexor and extensor muscles can cause pain, stiffness, and weakness in the elbow, forearm, wrist, and hand. Quite often these trigger point symptoms are mistaken for inflammation of the tendons which is what a true tennis/golfers elbow actually is. Failure to address the trigger points can lead to an incomplete recovery .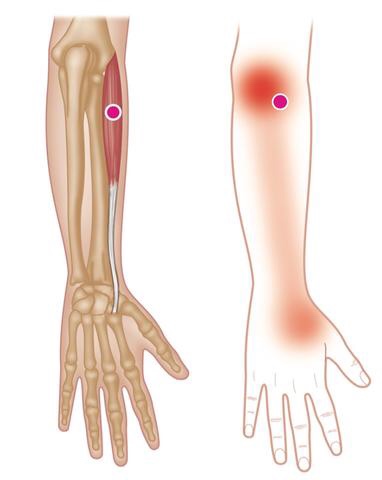
Trigger point massage
Session Description
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.
The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treate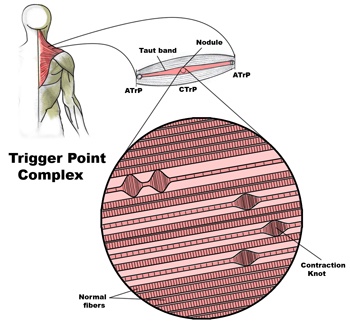
 d.
d.
Problems associated with trigger points
Trigger Points in muscle and other soft tissue are one of the most common causes of a wide variety of pain and dysfunction, including (but not limited to):
• Achy persistent pain
• Severe local pain
• Arm / leg pain
• Back pain
• Radiating pain
• Weakness
• Stiffness
• Pain resulting from a medical condition, such as
– Migraines
– Sciatica
– TMJ dysfunctions
– Arthritis
– Fibromyalgia
– Carpal tunnel syndrome
– Soft tissue injuries
– And more…
Trigger points in the levator scapula
The levator scapula is a muscle located in your neck. It originates on the transverse processes of C1-C4 vertebrae. It inserts on the superior part of the medial border of the scapula. This muscle acts to elevate the scapula and rotate the glenoid fossa downward. At the cervical attachment it acts to rotate the neck to the same side and assists extension. Trigger points will refer pain into the angle of the neck with spillover into the scapula. When this muscle is tight due to trigger points it will restrict neck rotation causing the classic stiff neck. With a forward head position this muscle often becomes stretched and over worked.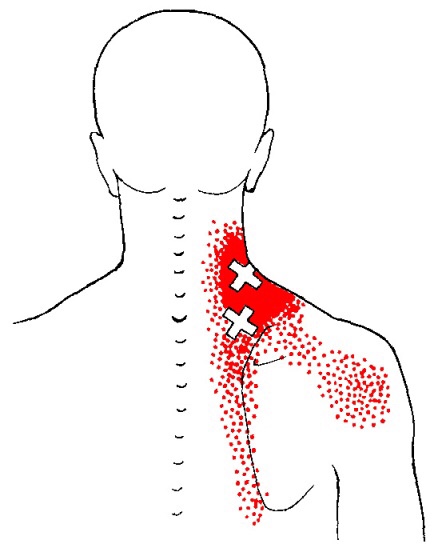
2 Critical Steps to Resolving Ankle Sprains

Efficient treatment of ankle sprains continues well after the pain subsides. While the majority of inversion (lateral) ankle sprains heal relatively quickly, up to 1/3 of patients, continue to note symptoms at one year, and up to 25% report pain, instability, crepitus, weakness, stiffness, or swelling at three years. (1) Re-injury is frequent, with rates reaching almost 75% in sports, like basketball. (2) Successful management of ankle sprains and prevention of re-injury are predicated on a couple of fundamental principles.
Management of ankle inversion sprains requires two steps; each is equally important.
- The first step entails the evaluation and treatment of acute pain.
- The second step involves preventing subsequent sprains – and new research validates the importance of chiropractic care to improve clinical outcomes in these recalcitrant cases.
STEP 1—Move for Pain Relief
Early return to activity for acute inversion sprains is supported by the literature. Exercises and treatments that promote joint motion and early return to weight bearing for acute ankle sprains have proven more effective than immobilization. While grade III sprains (ligament rupture) may require immobilization, grade I and II ankle sprains should forego complete immobilization and instead focus on regaining full range of motion. In fact, early rehab and return to weight bearing will increase ankle range of motion, decrease pain, and reduce swelling sooner than immobilization.
In a study by Linde et al., 150 patients with inversion ankle sprains were treated with early motion and weight bearing. After one month, 90% of the patients treated with early motion and weight bearing demonstrated pain-free gait and 97% had increased work ability. (3) Early mobility exercises would typically include:




These four exercises promote balance and range of motion – specifically dorsiflexion, which is a key contributor to ankle injury. Patients who have lost an average of 11 degrees of dorsiflexion are five times more likely to suffer lateral ankle sprains. (4)
In office care should also include mobilization and manipulation for restoring function. Joint mobilization has been shown to decrease pain, increase dorsiflexion, and improve ankle function. (5) IASTM or transverse friction massage to the affected ligament may help mobilize scar tissue and increase pliability. Myofascial release may help release tightness or adhesions in the gastroc and soleus. (Side note: The FAKTR concept seamlessly incorporates all of these tools to produce top-tier outcomes.)
Knowing when to treat and when to refer is critical. Whitman’s clinical prediction rule identifies four variables to predict the success of manipulation and exercise for the treatment of inversion ankle sprains. (6) The presence of three out of four of the following variables predict greater than a 95% success rate for manual therapy and exercise:
- Symptoms worse when standing
- Symptoms worse in the evening
- Navicular drop greater than 5 mm
- Distal tibiofibular joint hypomobility
STEP 2- Prevent Re-injury
The second step is shorter and easier than the first. The most crucial variable in the successful prevention of future ankle sprains is improving BALANCE. Balance training reduces the incidence of ankle sprains and increases dynamic neuromuscular control, postural sway, and joint position sense in athletes. (7) A study by de Vasconcelos et al. (2018) found that balance training reduced the incidence of ankle sprains by 38% compared with the control group. (7)
Two of the most common exercises used for balance and proprioception include the single-leg stance exercise and Veles. A simple explanation stressing the importance of balance training may be necessary to promote patient compliance.
Finally, encourage your patients start walking “normal” as soon as possible. As evidence-based chiropractors, we need to return patients back to their normal gait as soon as tolerable. Patients with foot and ankle pain will often favor a supinated gait in order to unload the soft tissues of the foot and arch in favor of their bony architecture on the lateral foot. The lateral column of the foot affords stability but at the expense of a very inefficient gait. Over an extended period, these patients may develop a Tailor’s bunion, i.e. 5th metatarsal head bursitis. However, in the case of ankle sprains, a rapid increase in activity may overload the metatarsal fast enough to cause a Jones Fracture. Return to normal gait will minimize these compensations.
Pregnancy Related Low Back Pain

Low back pain during pregnancy is quite common. In fact, between 50-75% of all pregnant women will experience low back pain. The pain is usually caused from rapid changes in weight, posture, gait and hormones.
The average woman gains between 20-40 pounds throughout pregnancy. This weight gain moves your center of gravity forward, causing your pelvis to tilt and your lower back to sway – placing excessive stress on the ligaments, discs, and joints of your spine.
 Pregnancy-related low back pain typically starts between the fifth and seventh month of pregnancy, although a significant portion of women experience pain sooner. Symptoms often begin at the base of your spine and may radiate into your buttock or thigh. Discomfort is often aggravated by prolonged standing, sitting, coughing, or sneezing. Your symptoms may increase throughout the day, and some patients report nighttime pain that disturbs their sleep. The extremes of activity seem to contribute to pregnancy-related low back pain – with increased risk for both “sedentary” and “physically demanding” lifestyles. Patients who have suffered with back pain prior to pregnancy are more than twice as likely to re-develop back pain during pregnancy.
Pregnancy-related low back pain typically starts between the fifth and seventh month of pregnancy, although a significant portion of women experience pain sooner. Symptoms often begin at the base of your spine and may radiate into your buttock or thigh. Discomfort is often aggravated by prolonged standing, sitting, coughing, or sneezing. Your symptoms may increase throughout the day, and some patients report nighttime pain that disturbs their sleep. The extremes of activity seem to contribute to pregnancy-related low back pain – with increased risk for both “sedentary” and “physically demanding” lifestyles. Patients who have suffered with back pain prior to pregnancy are more than twice as likely to re-develop back pain during pregnancy.
Be sure to tell your doctor if your symptoms include fever, chills, bleeding, spotting, unusual discharge, cramping, sudden onset pelvis pain, light-headedness, shortness of breath, chest pain, headache, calf pain or swelling, decreased fetal movement, or symptoms that radiate beyond your knee.
Unfortunately, pregnancy related low back pain occurs at a time when your medical treatment options are limited. Not surprisingly, over 90% of prenatal health care providers would recommend drug-free treatment, including the type of alternative therapy provided in this office. Studies have shown that chiropractic manipulation provides significant relief of pregnancy-related low back pain. Almost 75% of women undergoing chiropractic care report significant pain reduction with improved ability to function.
Most patients will also benefit from continuing aerobic exercise throughout pregnancy. The US Department of Health and Human Services advises that healthy pregnant women may begin or continue moderate intensity aerobic exercise for at least 150 minutes per week. Women should not begin “vigorous” exercise during pregnancy, but those who were preconditioned to vigorous exercise may continue. Be sure to check with your doctor prior to initiating or increasing any exercise program while you are pregnant.
Be sure to take frequent breaks from prolonged sitting or standing. You may find benefit by using a small foot stool to alternate feet while standing. Sleeping with a pillow between the knees in a side lying posture may help you to rest more comfortably. You should wear shoes with good arch supports. In some cases, your chiropractor may recommend a sacroiliac belt or pelvic support belt to help relieve your pregnancy-related low back pain.
Exercise of the Month – (Resisted Shoulder Retraction)
Resisted Shoulder Retraction
- Secure a piece of elastic resistance tubing to a doorframe.
- Sit or stand with your elbows tucked into your sides bent at 90 degrees, forearms pointing forward.
- Grasp the resistance band and pull it towards you by focusing on pinching your shoulder blades together.
- Return to the start position and repeat three sets of 10 repetitions daily or as directed.
*This exercise may also be performed using a cable row machine or by looping a piece of elastic resistance band over your feet while sitting on the floor with your legs directly in front of you.
Lumbar Radiculopathy? That sounds ridiculous!
Your nervous system is basically a big electrical circuit. Your spinal cord transmits all of the electrical nerve impulses between your brain and lower back. From there, individual nerves emerge from your spine then travel to supply sensation and movement to a specific area of your buttock, legs and/or feet. This allows you to move and feel sensations like touch, heat, cold and pain. Anything that

interferes with this transmission can cause problems.
You have been diagnosed with a “Lumbar Radiculopathy”. This means that one or more of the nerves emerging from your lower back has become irritated or possibly pinched. This often results in pain, numbness or tingling in the specific area of your leg that is supplied by the irritated nerve. The term “Sciatica” is often used to describe this condition, because most (but not all) “lumbar radiculopathies” involve the sciatic nerve which supplies the back & outside of your thigh and calf. Symptoms of a lumbar radiculopathy may vary from a dull ache to a constant severe sharp shooting pain. Your symptoms are likely aggravated by certain positions or movements.
To solve this problem, we will treat the source of your nerve irritation. It is important for you to follow your treatment plan closely and be sure to tell us immediately if you experience any progression of your leg pain, numbness or weakness.
Lumbar Degenerative Spondylolisthesis
Your lumbar spine (low back) is made up of five individual vertebra stacked on top of a bone called the sacrum. To allow for flexibility and movement, there is a cushion or “disc” in between each level. As we age, our discs and joints can wear and become thinner from a process called arthritis. This leads to additional changes, including loosening of the ligaments that hold your vertebra in place.

The term “degenerative lumbar spondylolisthesis” means that one of your vertebra has shifted forward on top of the one below as a result of arthritis and loosening ligaments. The condition usually comes on after age 50 and affects women six times more frequently than men. Degenerative spondylolisthesis occurs most commonly at your second lowest spinal level. (L4-5)
Sometimes, spondylolisthesis develops silently, but most patients report episodes of back pain that have occurred for many years. Patients often report increased pain when standing or when rising from a sitting position. Pain tends to increase throughout the day. If your nerve openings have become narrowed, the nerves may be pinched, and you may experience pain radiating into your legs. Leg symptoms that shift from side to side are characteristic of degenerative spondylolisthesis. Leg pain and tingling are fairly common, but be sure to tell your doctor if you notice more significant symptoms, like leg numbness, heaviness, weakness, loss of bowel or bladder function, or impotence.
Studies have shown no advantage for surgery over conservative care for most cases of degenerative spondylolisthesis. Approximately one-third of patients will experience progression of symptoms over time, and only 10-15% will ever need surgery to correct the problem. Fortunately, the majority of patients will benefit from treatment and exercises to help stabilize their spine.
You will need to perform your exercises consistently for sustained improvement. You should also try to add some type of aerobic exercise to your daily routine. Stationary cycling is a very good choice, and other options include water walking and swimming. Avoid wearing high heels. You may find some benefit for your arthritic symptoms by taking 1500mg of Glucosamine Sulfate each day. Using a hot pack for 10-15 minutes directly over your lower back may provide some benefit.
