The Lateral Pterygoid muscle is a muscle of the jaw. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate. It has its insertion on the condyloid process of the mandible. Functionally it it assists in opening the jaw by pulling the head of the mandibular condyle out of the mandibular fossa. Trigger points in this muscle refer pain into the temporal mandibular joint and maxillary sinus. Trigger points in this muscle are often the cause of pain felt from TMJ dysfunction.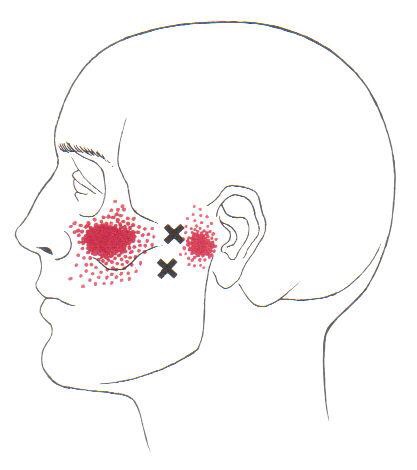
Massage
A treatment with Bryan Cobb RMT.
Session Description
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.
The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
What the Heck Is a Trigger Point?
By Bryan Cobb, Advanced Remedial Massage Therapist
What is a Trigger Point?
Trigger Points (TP’s) are defined as a “hyper-irritable spot within a taut band of skeletal muscle. The spot is painful on compression and can evoke characteristic referred pain and autonomic phenomena.”1
Put into plain language, a TP is a painful knot in muscle tissue that can refer pain to other areas of the body. You have probably felt the characteristic achy pain and stiffness that TP’s produce, at some time in your life.
TP’s were first brought to the attention of the medical world by Dr. Janet G. Travell. Dr. Travell, physician to President John F. Kennedy, is the acknowledged Mother of Myofascial Trigger Points. In fact, “Trigger Point massage, the most effective modality used by massage therapists for the relief of pain, is based almost entirely on Dr. Travell’s insights.”2 Dr. Travell’s partner in her research was Dr. David G. Simons, a research scientist and aerospace physician.
Trigger Points are very common. In fact, Travell and Simons state that TP’s are responsible for, or associated with, 75% of pain complaints or conditions.1 With this kind of prevalence, it’s no wonder that TP’s are often referred to as the “scourge of mankind”.
Trigger Points can produce a wide variety of pain complaints. Some of the most common are migraine headaches, back pain, and pain and tingling into the extremities. They are usually responsible for most cases of achy deep pain that is hard to localize.
A TP will refer pain in a predictable pattern, based on its location in a given muscle. Also, since these spots are bundles of contracted muscle fibres, they can cause stiffness and a decreased range of motion. Chronic conditions with many TP’s can also cause general fatigue and malaise, as well as muscle weakness.
Trigger Points are remarkably easy to get, but the most common causes are
•
TP’s (black dots) can refer pain to other areas (red)

Sudden overload of a muscle
• Poor posture
• Chronic frozen posture (e.g., from a desk job), and
• Repetitive strain
Once in place, a TP can remain there for the remainder of your life unless an intervention takes place.
Trigger Points Not Well Known
With thousands of people dealing with chronic pain, and with TP’s being responsible for — or associated with — a high percentage of chronic pain, it is very disappointing to find that a large portion of doctors and other health care practitioners don’t know about TP’s and their symptoms.
Scientific research on TP’s dates back to the 1700’s. There are numerous medical texts and papers written on the subject.
But, it still has been largely overlooked by the health care field. This has led to needless frustration and suffering, as well as thousands of lost work hours and a poorer quality of life.
How Are Trigger Points Treated?
As nasty and troublesome as TP’s are, the treatment for them is surely straight-forward. A skilled practitioner will assess the individual’s pain complaint to determine the most likely location of the TP’s and then apply one of several therapeutic modalities, the most effective of which is a massage technique called “ischemic compression”.
Basically, the therapist will apply a firm, steady pressure to the TP, strong enough to reproduce the symptoms. The pressure will remain until the tissue softens and then the pressure will increase appropriately until the next barrier is felt. This pressure is continued until the referral pain has subsided and the TP is released. (Note: a full release of TP’s could take several sessions.)
Other effective modalities include dry needling (needle placed into the belly of the TP) or wet needling (injection into the TP). The use of moist heat and stretching prove effective, as well. The best practitioners for TP release are Massage Therapists, Physiotherapists, and Athletic Therapists. An educated individual can also apply ischemic compression to themselves, but should start out seeing one of the above therapists to become familiar with
the modality and how to apply pressure safely.
1 Simons, D.G., Travell, D.G., & Simons, L.S. Travell and Simons’ Myofascial Pain and Dysfunction: the Trigger Point Manual.
Vol. 1. 2nd ed. Lippincott, Williams, and Wilkins, 1999.
2http://www.muscletherapyworks.com/MTW%20Biography%20T%20&%20S%2001.htm
Pregnancy Related Low Back Pain

Low back pain during pregnancy is quite common. In fact, between 50-75% of all pregnant women will experience low back pain. The pain is usually caused from rapid changes in weight, posture, gait and hormones.
The average woman gains between 20-40 pounds throughout pregnancy. This weight gain moves your center of gravity forward, causing your pelvis to tilt and your lower back to sway – placing excessive stress on the ligaments, discs, and joints of your spine.
 Pregnancy-related low back pain typically starts between the fifth and seventh month of pregnancy, although a significant portion of women experience pain sooner. Symptoms often begin at the base of your spine and may radiate into your buttock or thigh. Discomfort is often aggravated by prolonged standing, sitting, coughing, or sneezing. Your symptoms may increase throughout the day, and some patients report nighttime pain that disturbs their sleep. The extremes of activity seem to contribute to pregnancy-related low back pain – with increased risk for both “sedentary” and “physically demanding” lifestyles. Patients who have suffered with back pain prior to pregnancy are more than twice as likely to re-develop back pain during pregnancy.
Pregnancy-related low back pain typically starts between the fifth and seventh month of pregnancy, although a significant portion of women experience pain sooner. Symptoms often begin at the base of your spine and may radiate into your buttock or thigh. Discomfort is often aggravated by prolonged standing, sitting, coughing, or sneezing. Your symptoms may increase throughout the day, and some patients report nighttime pain that disturbs their sleep. The extremes of activity seem to contribute to pregnancy-related low back pain – with increased risk for both “sedentary” and “physically demanding” lifestyles. Patients who have suffered with back pain prior to pregnancy are more than twice as likely to re-develop back pain during pregnancy.
Be sure to tell your doctor if your symptoms include fever, chills, bleeding, spotting, unusual discharge, cramping, sudden onset pelvis pain, light-headedness, shortness of breath, chest pain, headache, calf pain or swelling, decreased fetal movement, or symptoms that radiate beyond your knee.
Unfortunately, pregnancy related low back pain occurs at a time when your medical treatment options are limited. Not surprisingly, over 90% of prenatal health care providers would recommend drug-free treatment, including the type of alternative therapy provided in this office. Studies have shown that chiropractic manipulation provides significant relief of pregnancy-related low back pain. Almost 75% of women undergoing chiropractic care report significant pain reduction with improved ability to function.
Most patients will also benefit from continuing aerobic exercise throughout pregnancy. The US Department of Health and Human Services advises that healthy pregnant women may begin or continue moderate intensity aerobic exercise for at least 150 minutes per week. Women should not begin “vigorous” exercise during pregnancy, but those who were preconditioned to vigorous exercise may continue. Be sure to check with your doctor prior to initiating or increasing any exercise program while you are pregnant.
Be sure to take frequent breaks from prolonged sitting or standing. You may find benefit by using a small foot stool to alternate feet while standing. Sleeping with a pillow between the knees in a side lying posture may help you to rest more comfortably. You should wear shoes with good arch supports. In some cases, your chiropractor may recommend a sacroiliac belt or pelvic support belt to help relieve your pregnancy-related low back pain.
Trigger points in the deltoid muscle
The deltoid is the main muscle that makes up the shoulder. It originates on the clavicle, acromion, and spine of the scapula. It inserts on the deltoid tuberosity of the humerus. The deltoid acts at the shoulder to produce abduction, and assist with flexion and extension. The deltoid is especially prone to developing trigger points. These posterior style will refer pain into the anterior and lateral shoulder. Trigger points in the posterior delt will refer pain into the posterior shoulder with spillover down the lateral arm.
Trigger points in the adductor pollicis
The adductor pollicis is a muscle in the hand and acts on the thumb. It originates on the transverse head of the third metacarpal, the oblique head of the base of the second and third metacarpals, and the trapezoid and capitate bones. It inserts on the base of the proximal phalanx and ulnar sesamoid. This muscle acts to adduct and flex the thumb. Trigger points cause pain and aching along the outside of the thumb and hand, spillover pain may reach the thenar eminence.
Lumbar Degenerative Spondylolisthesis
Your lumbar spine (low back) is made up of five individual vertebra stacked on top of a bone called the sacrum. To allow for flexibility and movement, there is a cushion or “disc” in between each level. As we age, our discs and joints can wear and become thinner from a process called arthritis. This leads to additional changes, including loosening of the ligaments that hold your vertebra in place.

The term “degenerative lumbar spondylolisthesis” means that one of your vertebra has shifted forward on top of the one below as a result of arthritis and loosening ligaments. The condition usually comes on after age 50 and affects women six times more frequently than men. Degenerative spondylolisthesis occurs most commonly at your second lowest spinal level. (L4-5)
Sometimes, spondylolisthesis develops silently, but most patients report episodes of back pain that have occurred for many years. Patients often report increased pain when standing or when rising from a sitting position. Pain tends to increase throughout the day. If your nerve openings have become narrowed, the nerves may be pinched, and you may experience pain radiating into your legs. Leg symptoms that shift from side to side are characteristic of degenerative spondylolisthesis. Leg pain and tingling are fairly common, but be sure to tell your doctor if you notice more significant symptoms, like leg numbness, heaviness, weakness, loss of bowel or bladder function, or impotence.
Studies have shown no advantage for surgery over conservative care for most cases of degenerative spondylolisthesis. Approximately one-third of patients will experience progression of symptoms over time, and only 10-15% will ever need surgery to correct the problem. Fortunately, the majority of patients will benefit from treatment and exercises to help stabilize their spine.
You will need to perform your exercises consistently for sustained improvement. You should also try to add some type of aerobic exercise to your daily routine. Stationary cycling is a very good choice, and other options include water walking and swimming. Avoid wearing high heels. You may find some benefit for your arthritic symptoms by taking 1500mg of Glucosamine Sulfate each day. Using a hot pack for 10-15 minutes directly over your lower back may provide some benefit.
Trigger points in the adductor longus.
The adductor longus is a muscle of the groin. It originates on the pubic body just below the pubic crest, and inserts on the middle third of the linea aspera of the femur. It acts on the hip joint to cause adduction and flexion. Distal Trigger points in this muscle refer pain to the upper medial knee and down the tibia. Proximal trigger points refer pain into the anterior hip. These trigger points are the most common muscular cause of groin pain. 
Lumbar Spondylolisthesis
Your spine is made up of 24 individual vertebrae all stacked on top of each other. The lowest five vertebrae are referred to as your lumbar spine. Each vertebra has two basic components: the “body” and the “arch.” You can envision this as a coffee mug lying on its side. The cup would represent the vertebral body, and the handle would represent the arch. The spinal cord travels through each of


the vertebral arches on its way from your brain to your tailbone. The term “lumbar isthmic spondylolisthesis” describes a condition where your arch has broken free from its anchor on the vertebral body, allowing the vertebral body to slide forward. Lumbar spondylolisthesis typically affects the lowest lumbar vertebra, L5, or occasionally the second lowest, L4.
The condition is sometimes caused by trauma, but more often follows a “stress fracture” involving the arch of the vertebra. This break and slippage is thought to result from repetitive movements, especially hyperextension (arching back) and rotation. The break usually happens during childhood but does not always cause symptoms when it occurs. Many times, the condition will lie dormant until later in life. Lumbar spondylolisthesis is present in six to seven percent of the population and affects males twice as often as females. The problem is more common in those who participate in sports. Some sports predispose children to this “break and slip”. Athletes who participate in gymnastics, rowing, diving, football, wrestling, weight lifting, swimming, tennis, volleyball, and track & field throwing sports (i.e. discus, shot put, etc) are at greatest risk.
The pain usually starts in your back but may radiate into your buttock or thigh. Your pain usually intensifies with standing upright for prolonged periods of time or leaning backwards, especially during heavy activity. Some women report increased symptoms during the later stages of pregnancy. Be sure to tell your doctor if you notice pain, numbness or tingling in your groin, a loss of bowel or bladder function, fever, night sweats, pain extending beyond your knee, or weakness in your legs.
Your doctor will “grade” your spondylolisthesis based on the percent of the vertebral body that has slipped forward. Your doctor will try to determine if your spondylolisthesis is “active”, meaning a recent break or “inactive”, referring to a long-standing problem. If your doctor has determined that your spondylolisthesis is new and has a chance of worsening, you may need to stop certain activities or sports for a period of time until your fracture heals. Sometimes a lumbar brace is used to help you recover more quickly. Patients with a long-standing “inactive” spondylolisthesis may benefit from a combination of treatments including stretching and strengthening. You should limit leaning backwards or sleeping on your stomach. Females should avoid wearing high heels.
How Does Chiropractic Help With Headaches?

How Does Chiropractic Help with Headaches?
Since 9 out of 10 Americans suffer from some form of headache, we tend to think of them as just a nuisance that can be relieved by taking a painkiller or a nap. Those solutions sometimes lighten the pain momentarily, but recurring headaches are a symptom that something else is wrong, and finding the root cause of your headaches is imperative to putting an end to them.
Fortunately, there’s a proven alternative. According to a new study, chiropractic treatment can provide “immediate relief” for many headache patients.
The majority of primary headaches, including tension headaches and migraines, are frequently associated with muscle tension or joint restrictions in the neck. These problems occur more often than ever before because nowadays we’re sitting in front of the computer for hours at a time or looking down at a phone to surf the web or text.
Chiropractors work to remove the triggers of these painful problems like stiffness, tightness, inflammation, and nerve irritation in the cervical spine. In addition to performing gentle spinal manipulation and soft tissue release, your chiropractor can also provide nutritional advice to help you avoid common migraine triggers found in your diet. Many patients also benefit from chiropractic advice on posture, relaxation techniques, and exercises to help prevent future problems.
So, if you or someone you know suffers from headache, call our office today. And check out this short video for more information about relief for neck-related headaches.
Pregnancy Related Low Back Pain
Pregnancy-related LBP
Researchers estimate that between 45-75% of pregnant women will experience low back pain at some stage of their pregnancy. (1-5) Up to 33% rate their pain as severe. (6) Pregnancy-related low back pain (P-LBP) leads to lower quality of life, restricted activity, and disability – with almost 25% of pregnant women taking sick leave for LBP. (2,7-11) The recurrence rate for pregnancy-related low back pain is 85-90%. (11-14) Consequently, almost 1 in 5 women who report P-LBP during an initial pregnancy will avoid future pregnancies due to fear of returning symptoms. (15)
Pharmacologic options during pregnancy are limited, however a new study highlights a conservative alternative. A December 2017 systematic review of 102 studies found moderate-quality evidence suggesting manipulation had a significant effect on decreasing pain and increasing functional status in pregnant and post-partum women with LBP. (16)
This concurs with prior research showing that almost 75% of women undergoing chiropractic manipulation report significant pain reduction and clinically significant improvements in disability. (17,18) Postpartum LBP also responds favorably to spinal manipulation – approximately 10 times better than watchful waiting. (19)
Our providers strive to deliver safe and effective evidence-based care for your patients. Incorporating gentle manipulation with the appropriate exercises generally provides significant relief in very few visits.
