A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
Hip Pain
Diagnosis of trigger points.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
What is a trigger point
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
Snapping Hip. Not as horrific as it sounds.
The muscle responsible for flexing your hip toward your trunk, is called the Psoas. This muscle begins on your lower spine and passes through your pelvis to attach onto the top of your femur (thigh bone). Along this course, the muscle travels across the front of your hip socket and over several bony prominences. If the muscle is too tight, its tendon may rub over these “bumps”. This occasionally produces an audible snapping sound, hence the moniker, “snapping hip”, aka “psoas tendinopathy”.
 The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
Your symptoms may include a “snapping” sound or sensation when you flex and extend your hip- although many cases are silent. Repeated rubbing causes inflammation and subsequent deep groin pain that can radiate to the front of your hip or thigh. Long-standing problems can trigger weakness or even limping.
The diagnosis of snapping hip is frequently overlooked. In fact, some studies show that identification is often delayed more than two years, while other potential causes are pursued. Fortunately, your problem has been recognized, and our office has several treatments to help you recover.
Psoas problems often start when one group of muscles is too tight, while another is too loose. Your home exercises will help to correct this problem. Depending upon the severity of your condition, you may need to avoid certain activities for a while. You should especially avoid repetitive hip flexion. Prolonged seated positions can encourage shortening of your hip flexors so be sure to take frequent breaks. Patients with fallen arches may benefit from arch supports.
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
The Bird Dog

Today we are going to look at one of the most effective exercises to protect your lumbar spine from discogenic injury, the bird dog. A great way to work on both posterior chain and rotational stability, the bird dog is safe, effective and simple.
- Get on your hands and knees (four point position) with your knees and hands, hip and shoulders width apart.
- Your back is in neutral position (slightly arched) and your chin must be tucked in.
- Activate your lower abdominals (transversus abdomini) by bringing your belly button inward and by activating your pelvic floor muscles 20 to 30% of maximal contraction.
- Maintain a steady abdominal breathing while you simultaneously lift one leg backwards and the opposite arm overhead keeping your back in neutral position.
- Return to the initial position and repeat with the other leg and arm.
2 sets of 10 reps as part of your regular core/stability routine will have you well on your way to a life-proof low back!
Image and instructions from physiotec.ca
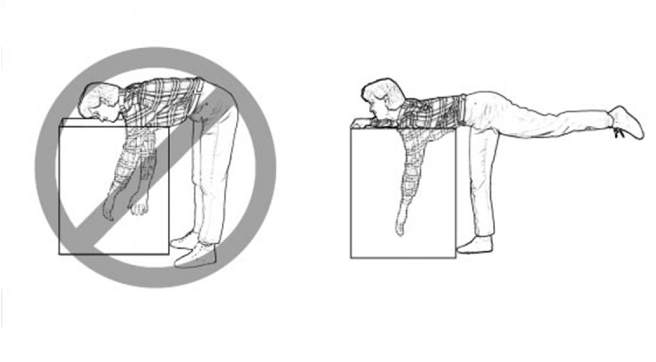
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
Our Condition of the Month: ITB Syndrome
Iliotibial Band Syndrome
Your iliotibial band is a fibrous band of tissue running from the crest of your hip, down to your knee. A muscle near the crest of your hip called the tensor fascia lata, attaches to this band to help control movements of your leg. Your iliotibial band passes over the point of your hip and over another bony bump on the outside of your knee called the lateral epicondyle. When the band is too tight, it can become painfully inflamed as it repeatedly rubs over the top of either of these bony projections. Irritation at the bony bump near the knee is called iliotibial band friction syndrome.
The condition usually presents as pain on the outside of your knee that becomes worse with repetitive knee flexion or extension. This condition is the leading cause of lateral knee pain in runners, especially slower “joggers.” The pain usually develops 10-15 minutes into the workout. You may sometimes feel or hear a click during movement. Symptoms generally ease at rest. Running on slick “wintry” surfaces may aggravate the condition. Excessively worn running shoes may be a culprit.
This problem is commonly caused by weakness in your gluteal muscles. When these muscles are weak, the muscle that attaches to your iliotibial band must contract harder to stabilize your hip. Having one leg longer than another is a known aggravating factor.
Runners should minimize downhill running and avoid running on a banked surface like the crown of a road or indoor track, as well as wet or icy surfaces. Runners should reverse directions on a circular track at least each mile. Bicyclists may need to adjust seat height and avoid “toe in” pedal positions. Avoid using stair climbers or performing squats and dead lifts. Sports cream and home ice massage may provide some relief of symptoms.
Lifting Mechanics Made Simple

Here are some tips to help you lift safely:
✓ Avoid lifting or flexing before you’ve had the chance to warm up your muscles (especially when you first awaken or after sitting or stooping for a period of time).
✓ To lift, stand close directly facing object with your feet shoulder width apart.
✓ Squat down by bending with your knees, not your back. Imagine a fluorescent light tube strapped to your head and hips when bending. Don’t “break” the tube with improper movements. Tuck your chin to help keep your spine aligned.
✓ Slowly lift by thrusting your hips forward while straightening your legs.
✓ Keep the object close to your body, within your powerzone” between your hips and chest. Do not twist your body, if you must turn while carrying an object, reposition your feet, not your torso.
An alternative lifting technique for smaller objects is the golfers lift. Swing one leg directly behind you. Keep your back straight while your body leans forward. Placing one hand on your thigh or a sturdy object may help.
Hip Abductor Weakness

* The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance.
* Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity.
* There is no “typical” presentation for hip abductor weakness, but the problem must be considered in any patient with lower chain symptomatology, particularly those with hip tendinopathy, greater trochanteric pain syndrome, iliotibial band syndrome, patellofemoral pain syndrome, ACL injury, medial knee pain, and lower back pain.
*Hip abductor weakness is often accompanied by lower crossed syndrome – a larger pattern of biomechanical dysfunction involving weakness of the abdominal wall and hypertonicity in the hip flexors and paraspinal musculature. Evaluation should include a relatively global assessment of lumbopelvic muscle and joint function. Additionally, clinicians should assess for the presence of foot hyperpronation in patients with hip abductor weakness.
