The lateral pterygoid muscle plays an important role in prober jaw function. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate, and inserts on the condyloid process of the mandible. It’s action is to pull the head of the mandibular condyle out of the mandibular fossa while opening the jaw. When trigger points develop they refer pain into the temporal mandibular joint and maxillary sinus. This referral is commonly mistaken for TM arthritis. In addition to the referral pain, trigger points in this muscle can also effect proper movement of the jaw.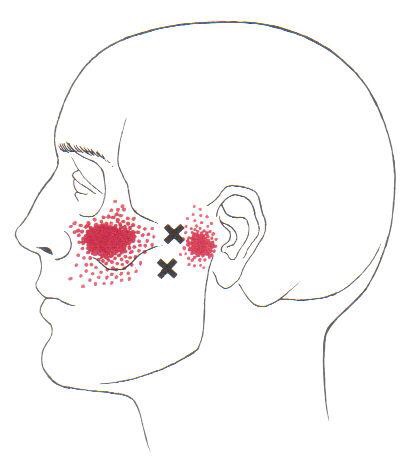

Health
FAI starts you on the road to failure.
Your hip socket or “acetabulum” is covered by smooth, glassy cartilage extending all the way to its outer rim. The term “Femoroacetabular impingement” (FAI) means that this rim of cartilage is being pinched when you move your hip into certain positions. Repetitive pinching results in irritation, tearing, or even detachment of this cartilage from your hip socket.

FAI occurs because of a mismatch between the head of your femur and the socket of your hip. The mismatch may be from an abnormally shaped hip bone (cam deformity), or having too much cartilage on the rim of your hip socket (pincer deformity). Most frequently, FAI results from a combination of both (combined or mixed deformity).
FAI is most common in young active people. Although the deformity may be present on both sides, symptoms are usually one-sided. The condition is equally common among men and women. Symptoms of FAI include a constant dull pain with periods of sharp pain, made worse by activity. Walking, pivoting, prolonged sitting, stair climbing, and impact activities like running or jumping can aggravate your symptoms. Snapping, locking, and clicking are common.
Our office will help direct a rehab program to maximize your chance of recovery. You should attempt to stay active, but avoid activities that aggravate symptoms. You may consider temporarily switching to low-impact activities, like stationary biking or water-walking. You should avoid motions that combine flexion and internal rotation, like- getting out of a car with one leg at a time, swimming the breaststroke, or performing squats. Patients with FAI should avoid excessive stretching, as this could aggravate the condition, but will likely benefit from strengthening exercises in the type of treatment provided in this office.
An Open Letter to our Medical friends.

In the past year, many trusted medical establishments including the FDA (1), CDC (2), Joint Commission (3,4), JAMA (5), and The American College of Physicians/ Annals of Internal Medicine (6) have encouraged medical providers to prescribe spinal manipulation as a first line treatment for acute, subacute, and chronic low back pain.
Most recently, The Lancet echoed that endorsement, and provided a unique perspective:
The reduced emphasis on pharmacological care recommends nonpharmacological care as the first treatment option and reserves pharmacological care for patients for whom nonpharmacological care has not worked. These guidelines endorse the use of exercise and a range of other non- pharmacological therapies, including massage, spinal manipulation, and acupuncture.
Gaps between evidence and practice exist, with limited use of recommended first- line treatments and inappropriately high use of imaging, rest, opioids, spinal injections, and surgery. Doing more of the same will not reduce back-related disability or its long-term consequences. The advances with the greatest potential are arguably those that align practice with the evidence. (7)
Unfortunately, personal experience skews our perception of each other’s merit, i.e., we primarily see each other’s failures since the successes don’t need to seek additional care. Regardless of our professional degree, we all have failed cases mixed into our many clinical successes. We must not lose sight of the evidence supporting each other’s overwhelming proven value for a given diagnosis. If we judge each other by our successes rather than our failures, we will work toward an integrated model where the patient wins. Together, we will help more patients than either working alone.
We are honored for the opportunity to co-manage your patients.
References
1. FDA Education Blueprint for Health Care Providers Involved in the Management or Support of Patients with Pain. May 2017. Accessed on May 12, 2017
2. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain- United States, 2016. MMWR Recomm Rep 2016;65(No. RR-1):1–49.
3. The Official Newsletter of The Joint Commission. Joint Commission Enhances Pain Assessment and Management Requirements for Accredited Hospitals. July 2017 Volume 37 Number 7. Ahead of print in
2018 Comprehensive Accreditation Manual for Hospitals.
4. Joint Commission Online. Revision to Pain Management Standards. http://www.jointcommission.org/assets/1/23/jconline_november_12_14.pdf
5. Paige NM, Miake-Lye IM, Booth MS, et al. Association of Spinal Manipulative Therapy With Clinical Benefit and Harm for Acute Low Back Pain; Systematic Review and Meta-analysis. JAMA. 2017;317(14):1451-1460.
6. Qaseem A, et al. for the Clinical Guidelines Committee of the American College of Physicians. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514-530.
7. Foster, Nadine EBuchbinder, Rachelle et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet, Published Online March 21, 2018 http://dx.doi.org/10.1016/ S0140-6736(18)30489-6
I’ve never baked anything in my life; how do I have a Baker’s Cyst?
Your body has strategically-placed, fluid-filled cushions called “bursa” around each joint. Bursa act to reduce friction where muscular tendons rub on bone. Your knee is surrounded by several bursa that share fluid with the inside of your knee joint and with each other. You can think of this like a chain of lakes connected by streams. If the inside of your knee joint or any of the bursa around your knee becomes inflamed, the entire system fills. When swelling exceeds each individual bursa’s capacity, this fluid creates a soft balloon-like swelling of the popliteal bursa behind your knee called a “Popliteal cyst”, or more commonly a “Baker’s cyst”.
 This swelling is usually not from a problem with the popliteal bursa itself, but rather, inflammation somewhere else in the joint that has distended the popliteal bursa. This swelling is often the result of arthritis or damage to a ligament or cartilage within the knee.
This swelling is usually not from a problem with the popliteal bursa itself, but rather, inflammation somewhere else in the joint that has distended the popliteal bursa. This swelling is often the result of arthritis or damage to a ligament or cartilage within the knee.
A Baker’s cyst is often painful, and the discomfort may increase when you attempt to move your knee. Depending on the severity of your swelling, your symptoms may vary between a feeling of fullness and significant pain. It is not unusual for a Baker’s cyst to change in size from day to day, depending on the amount of swelling. Be sure to tell us if your pain progressively increases when you walk or if you notice warmth, redness or swelling in your calf, as these could be signs of a more significant problem.
Sometimes rest and elevation of your leg help to alleviate pain and swelling. Initially, you may need to avoid activities, like squatting, kneeling, heavy lifting, climbing stairs, or running. Wearing a brace on your knee may compress the cyst and cause an increase in your pain. Since Baker’s cysts are generally a problem that is secondary to another condition, treatment is most effective when directed at the underlying problem.
Spring Cleaning Tips
If you plan on doing a bit of spring cleaning soon, here is our friendly safety reminder: Don’t forget that some chores are a workout, so stretch accordingly before and after. Also, be mindful of your posture throughout your cleaning.
Keep a neutral spine, bend at your knees when lifting heavy items, and never twist your back at unhealthy angles.
Trigger points in the serratus anterior
The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
There is nothing great about greater trochanteric pain syndrome. Nothing at all.
Your hip typically has about six small fluid-filled sacs called “bursa” that act as cushions between tendons and bone. One of the most common causes of hip pain is a condition called, “hip bursitis” which means that one or more of your bursas have become painfully inflamed. The broader (more accurate) diagnosis of “Greater trochanteric pain syndrome” (GTPS) describes an uncomfortable collection of problems affecting the outermost portion of your hip. GTPS can include swelling of one or more of the fibrous tendons that attach your muscles onto your hip – a condition called, “tendinitis.” In addition to bursitis & tendonitis, GTPS may originate from tightness in the muscle that travels over your hip en route to your knee- resulting in compression and irritation to your hip.

Greater trochanteric pain syndrome is most common in middle age to elderly adults and is 2-4 times more common in females. Sometimes the problem affects both hips at the same time. Approximately 1/3 of patients with GTPS have lower back pain. Patients who have arthritis in their hips and knees are more likely to suffer from ongoing complaints.
Your symptoms probably include a persistent pain on the outside of your hip, buttock, and upper thigh. Your discomfort may be aggravated by sitting with your leg crossed, arising from a seated position, prolonged standing, climbing stairs, and high-impact activities, like running. Sometimes patients find it difficult to sleep, since lying on the painful hip usually increases symptoms.
For adults, x-rays may or may not be needed to confirm the diagnosis, but children and adolescents usually require films to rule out more serious childhood diseases. Be sure to tell your doctor if you notice that you have a fever, leg numbness, pain radiating significantly beyond your knee, or pain in the front of your groin crease (the area where you leg meets your pelvis.)
Conservative treatment, like the type provided in this office, is successful in about 90% of cases. If you have acute pain, you may need to temporarily limit or discontinue activities that increase your discomfort. Using ice or ice massage at home may help. Some patients find temporarily relief by applying sports creams. Very commonly, patients with pain on the outside of their hip suffer from weakness in one of their buttock muscles, called the “gluteus medius.” When this muscle lacks strength, it is unable to protect your hip during normal activities, like walking. Research has shown that strengthening your hip has a dramatic effect on your progress.
Athletes should avoid running on a banked surface, like the crown of a road or indoor track. Be sure to reverse directions each mile if you run on a circular track. Avoid running on wet or icy surfaces, as this can cause increased tension in your hip. Runners with a “lazy” narrow-based running gait will benefit by increasing their step width to minimize stress on their hip. Cyclists need to make sure that their seat is not positioned too high. Overweight patients should consider weight reduction programs.
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.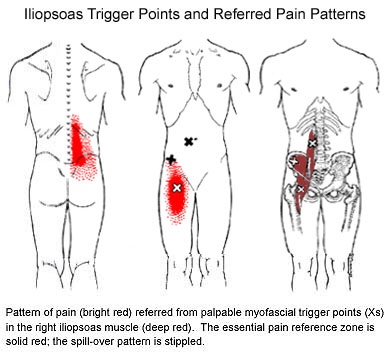
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 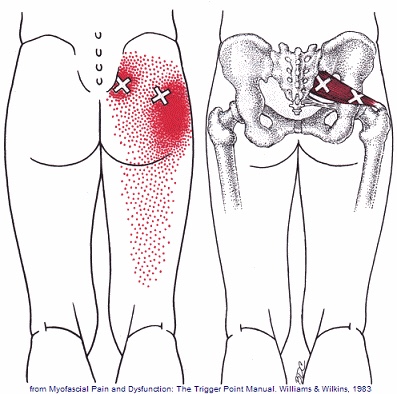
Piriformis Syndrome; a real bummer.
Piriformis syndrome results from compression of the sciatic nerve as it passes underneath a muscle in your buttock called the piriformis. Your piriformis muscle attaches from the lowest part of your spine (sacrum) and travels across to your hip. The muscle helps to rotate your leg outward when it contracts. In most people, the sciatic nerve travels deep to the piriformis muscle.

When your piriformis muscle is irritated or goes into spasm, it may cause a painful compression of your sciatic nerve. Approximately ¼ of the population is more likely to suffer from piriformis syndrome because their sciatic nerve passes through the muscle.
Piriformis syndrome may begin suddenly as a result of an injury or may develop slowly from repeated irritation. Common causes include: a fall onto the buttocks, catching oneself from a “near fall,” strains, long distance walking, stair climbing or sitting on the edge of a hard surface or wallet. In many cases, a specific triggering event cannot be pinpointed. The condition is most common in 40-60 year olds and affects women more often than men.
Symptoms of piriformis syndrome include pain, numbness or tingling that begins in your buttock and radiates along the course of your sciatic nerve toward your foot. Symptoms often increase when you are sitting or standing in one position for longer than 15-20 minutes. Changing positions may help. You may notice that your symptoms increase when you walk, run, climb stairs, ride in a car, sit cross-legged or get up from a chair.
Sciatic arising from piriformis syndrome is one of the most treatable varieties and generally is relieved by the type of treatment provided in this office. You may need to temporarily limit activities that aggravate the piriformis muscle, including hill and stair climbing, walking on uneven surfaces, intense downhill running or twisting and throwing objects backwards, i.e., firewood. Be sure to avoid sitting on one foot and take frequent breaks from prolonged standing, sitting and car rides. You may find relief by applying an ice pack to your buttock for 15-20 minutes at a time, several times throughout the day.
