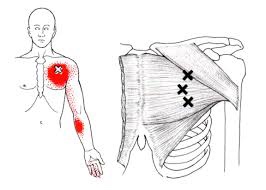
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Chronic Pain
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
CTS at Night.
For those who have carpal tunnel syndrome (CTS), it’s no surprise that CTS is frequently most expressive during the night, often to the point of interrupting sleep and/or making it difficult to fall back to sleep. So why is that?
The primary reason for nighttime CTS symptoms has to do with the wrist, as it is very difficult to sleep with the wrist held in its “ideal” or least irritating position. In fact, most people favor “curling” the back of the hand under the chin or bending the hand/wrist backwards under the head. When the wrist is bent in either direction, it can increase the pressure inside the wrist, which can generate the various symptoms associated with CTS.
One study evaluated the pressure inside the carpal tunnel while participants slowly moved their wrists. The researchers found many movements didn’t need to exceed 20 degrees before the pressure increased enough within the carpal tunnel to generate symptoms.
Because it doesn’t take a lot of movement to build up excessive pressure in the wrists of those with CTS, many doctors recommend the use of a “cock-up splint” for the non-surgical treatment of CTS in order to help keep the wrist in a neutral position.
Wrist posture is also an important factor during the day. One study looked at typing on a tablet PC, which allowed people to work in non-traditional settings. As screen size reduced, the posture required to type became more limited and accelerated the usual rate of pain onset in the neck, elbows, and wrists.
This study also looked at three different positions used when working on touch-screen devices: desk, lap, and bed. The healthy subjects completed six, 60-minute typing sessions using three virtual keyboard designs: standard, wide, and split. The researchers monitored the position of the wrist, elbow, and neck while the participants typed and followed up each session with questionnaires designed to measure discomfort.
The research team reported that typing in bed required greater wrist extension but resulted in a more natural elbow position than typing at a desk. The angled split keyboard significantly reduced the wrist deviation vs. the standard or wide keyboard designs. All three regions—the neck, elbow, and wrist—exhibited more movements (13% to 38%) towards the end of the one hour sessions, which correlated with a significant increase in pain in every body region investigated. Overall, using a wider keyboard while sitting at a desk was the most tolerable position among study participants.

How can I calm down my WAD symptoms?

Whiplash is really a slang term for the rapid back and forth whipping of the head on the neck, usually associated with motor vehicle accidents. The title “Whiplash Associated Disorders”, or WAD, describes it best because it includes ALL of the MANY signs and symptoms of the disorder.
WAD basically comes in three sizes based on the degree of injury. A WAD I is present when there is pain but no physical examination findings; WAD II occurs when there are exam findings but no neurological loss (numbness or weakness); and WAD III includes loss of neurological function. There is also a separate WAD level that includes fractures and dislocations (WAD IV).
There are many things that can be done by the patient to assist in the healing process for WAD. The first well-studied recommendation is to “continue with your usual activities.” Try to keep active and not change your routine. The good news is that WAD (especially types I and II) usually resolves without complication, and recovery is even more likely to occur if you don’t deviate much from your routine.
For those whose symptoms are more severe and/or not resolving, mobilization and manipulation of the neck and back are very effective treatment options. In addition to treatments you’d receive in a chiropractic office, there are MANY things you can do at home as “self-help strategies.” Some of these include (“PRICE”):
1) PROTECT: Though it’s important to continue with your usual daily activities, this is dependent on both the degree of tissue injury and your pain tolerance. So do as many of your usual daily activities as possible, but AVOID those that result in a sharp, lancinating type of pain or those where recovery from the pain is delayed. Therefore, this category may require modifying your ADLs (activities of daily living). A cervical collar (hard orsoft) should NOT to be used UNLESS you have an unstable injury (fracture or a grade III sprain).
2) REST: Doing too much is like picking at a cut (which can delay healing) and doing too little can lead to a delayed healing response as well. Staying within reasonable pain boundaries is a good guide.
3) ICE > HEAT: Ice reduces swelling, and your doctor will typically recommend it over applying heat, especially on a recent injury. Heat draws fluids in, and while it may feel good, it can make your symptoms worse.
4) COMPRESS: We can basically ignore this when referencing neck pain. This pertains better to wrapping an ankle, knee, wrist, or elbow with an elastic compression orthotic or brace.
5) ELEVATE: This too is meant for the acute stages of an extremity injury like a foot or ankle.
Exercises unique for neck pain in the acute, subacute, and chronic stages of healing are perhaps the most important of the self-help approaches. In the ACUTE phase, try these…
1) Range of Motion: Once again, stay within “reasonable pain boundaries” as you move your head forwards, backwards, side to side, and rotate left and right. These can be done either with or without LIGHT resistance applied using one or two fingers placed against your head. Limit the repetitions to three slow reps in each direction and emphasize the release of the movement.
2) Chin/head Glides: Tuck in the chin (think of creating a double or triple chin) followed by poking the chin/head out.
In the SUBACUTE and CHRONIC phases of healing, the importance of strengthening the deep neck flexors cannot be over emphasized. Please refer to last week’s article for a description of this (see #3 of the 6 recommendations listed).
When Are My Shoes “Done”?

Running shoes need to be replaced every 250 miles. There are three basic options:
✓ Motion Control Shoes – Designed for people with low or no arches, these shoes are for runners who strike the ground on the outer edge of their foot. Avoid overly stiff shoes as these decrease you perception of ground strike and lead to new injuries.
✓ Stability or Neutral Shoes – Designed for people with normal or average arches and running mechanics. The shoe contains some cushioning to absorb shock and prevent injuries and some rigidity to avoid pronation.
✓ Cushioned Shoes – Designed for people with high arched feet. Their footprint will typically leave a thin band along the foot’s edge. As they run weight is distributed from heel strike to the outer edge of the foot and small toes that bear the brunt of “lift off.” This shoe is more flexible and absorbs the shock created by the lack or rotation (under-pronation) created by their running style.
Workers compensation cases highlight the value of chiropractic care

A newly published analysis of 5511 workers compensation cases highlights the value of chiropractic care: “those injured workers who first saw a chiropractor experienced shorter first episodes of compensation (vs. physical therapy alone)”.
If you or someone you know has suffered a job-related injury, call us today. Our goal is to provide the most effective care that gets you back to work ASAP!
Do you have Carpal Tunnel Syndrome?
Carpal Tunnel Syndrome is VERY common. If fact, it affects 3-6% of the general population, and up to 50% of those afflicted have it in both hands! So what makes it so common? Here are several reasons:
1) ANATOMY: The wrist is made up of eight small “carpal” bones that allow the wrist to bend and twist in many different positions. If you were to look at the wrist “head on,” you’d notice it is shaped like a tunnel where the eight little carpal bones make up the “roof” and the transverse carpal ligament is the “floor.” You’ll also notice nine tendons and their sheaths that pass through the carpal tunnel and attach the forearm muscles to the fingers on the palm side of the arm, blood vessels, and the median nerve. When there is less available space within the carpal tunnel (due to inflamed tendons, for example), the added pressure can compress the median nerve and result in numbness, tingling, and weakness, mostly into the second to fourth fingers.
2) JOBS: People with occupations that require fast, repetitive movements and/or a firm grip with little rest have a higher likelihood of developing CTS.
3) GENDER: Women have a greater risk of developing CTS than men due to smaller wrists and hormonal changes that may result in swelling in the wrist.
4) AGE: Individuals over age 50 have a greater risk of developing CTS, especially females.
5) GENERAL HEALTH ISSUES: There are a host of conditions that can cause and/or aggravate CTS. Some of these include rheumatoid arthritis, diabetes, osteoarthritis, low thyroid function, and space-occupying issues like a ganglionic cyst inside the tunnel. Certain medications, such as birth control pills, and some forms of chemotherapy can also cause CTS. A pinched nerve in the neck or shoulder can alter median nerve function, which can exacerbate CTS symptoms.
6) TRAUMA: A fall onto an outstretched arm can sprain and/or fracture the wrist. If a fracture occurs, the onset of CTS can be very rapid, and quick realignment of the fracture is very important.
Chiropractic care offers a non-surgical solution to CTS, which includes splinting (primarily at night and when driving but usually less often during the day as we tend to “fight” against the splint), anti-inflammatory measures (ice, nutrients such as ginger, turmeric, bioflavonoids), and manual therapies—manipulation of the fingers, hand, wrist, elbow, shoulder, and neck (as indicated) and muscle release techniques to the forearm are very helpful. There are also effective exercises that patients can do at home that include joint range of motion and muscle stretching techniques.

Trigger points in the trapezius muscle.
The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
How long does Whiplash last?

First, what is whiplash? It’s a lot of things, which is why the term WAD or Whiplash Associated Disorders has become the most common term for the main signs and symptoms associated with a whiplash injury. WAD is usually associated with a motor vehicle collision, but sports injuries, diving accidents, and falls are other common ways to sustain a WAD injury.
To answer the question of the month, in most cases, the recovery rate is high and favors those who resume their normal daily activities. The worse thing you can do when you sustain a WAD injury is to not do anything! Too much rest and inactivity leads to long-term disability. Of course, this must be balanced with the degree of injury, but even when the injury requires some “down time,” stay as active as possible during the healing phase.
Many people recover within a few days or weeks while a smaller percentage require months and about 10% may only partially recover. So what can be done to give you the best possible chance to fully recover as soon as possible?
During recovery, you can expect your condition to fluctuate in intensity so “listen” to your body, let it “guide” you during activity and exercise, and stay within “a reasonable boundary of pain” during your activity. Remember, your best chance for full recovery FAVORS continuing a normal lifestyle. Make reasonable modifications so you can work, socialize, and do your “normal” activities!
The KEY: Stay in control of your condition – DO NOT let it control you! Here are some tips:
1) POSTURE CONTROL: Keep the weight of the head back by gliding your chin back until you “hit” a firm end-point. Then release it slightly so it’s comfortable—this is your NEW head position!
2) FLEXIBILITY: Try this range of motion (ROM) exercise… Slowly flex your neck forwards and then backwards, then bend your neck to the left and then the right, and then rotate it to the left and to then to the right. THINK about each motion and avoid sharp, knife-like pain; a “good-hurt” is okay! Next, do the same thing with light (one-finger) resistance in BOTH directions. Try three slow reps four to six times a day!
3) MUSCLE STRENGTH: Try pushing your head gently into your hand in the six directions listed above to provide a little resistance. Next, reach back with both hands or wrap a towel around your neck and pull forwards on the towel while you push the middle of your neck backwards into the towel doing the chin-tuck/glide maneuver (same as #1). Repeat three to five times slowly pushing, and more importantly, release the push slower! This is the MOST IMPORTANT of the strengthening exercises in most cases! Next, “squeeze” your shoulder blades together followed by spreading them as far apart as possible (repeat three to five times).
4) PERIODIC BREAKS: Set a timer to remind yourself to do a stretch, get up and move, to tuck your chin inwards (#1) and do some of #2 and #3 every 30-60 minutes.
5) LIFTING/CARRYING/WORK: Be SMART! Do not re-injure yourself. Change the way you handle yourself in your job, in the house, and while performing recreational activities.
6) HOUSEHOLD ACTIVITIES: Use a dolly to move boxes and keep commonly used items within easy reach (not too high or low).
Be smart, stay educated, work within the range your body tells you is “safe” and most importantly, STAY IN CONTROL!!!
My back hurts, why look at my feet?
Improperly supported feet can affect the alignment of all of the structures above. To improve your overall comfort:
✓ Choose shoes with good arch support.
✓ Avoid going barefoot or wearing shoes that lack support (i.e. flip-flops). The following brands of sandals provide better than average arch support: Naot, Fit Flops, Orthoheels, Abeo, Vionic and Yellow box.
✓ Avoid high-heeled shoes or boots (keep heels to a maximum of 1½ inches, especially if you are going to be doing a lot of walking).
✓ “Cross-trainer” athletic shoes tend to provide the best all around support and shock absorption for daily activities.
✓ Patients with fallen arches should consider adding arch supports or orthotics.
✓ Repair or replace shoes with worn soles or heels.
