The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 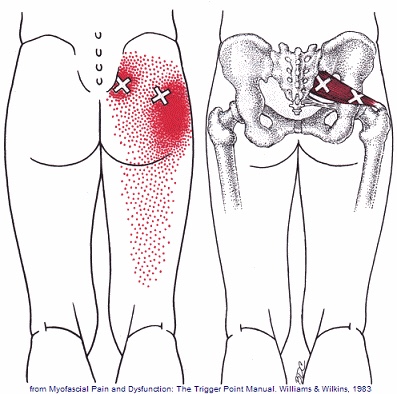
Chiropractic
Scapular Dyskinesis (Yes, its a thing).
Your shoulder is formed by three bones; the scapula (shoulder blade), the clavicle (collar bone), and the humerus (long arm bone.) These bones come together to form a shallow ball & socket that relies upon the surrounding muscles for support. All of your shoulder muscles must work in a coordinated fashion to have a healthy and stable joint. Disruption of the normal rhythm of your shoulder blade creates abnormal strain on your shoulder and rotator cuff called “Scapular dyskinesis”. This dysfunction crowds the area of your shoulder where your rotator cuff tendons live and may create a painful pinching of your tendons or bursa each time you raise your arm. Many shoulder problems, including sprains/strains, tendinitis, bursitis, or rotator cuff irritation, result from this often overlooked culprit.

Scapular dyskinesis most commonly originates from weakness or imbalance of the muscles that control your shoulder blade. Sometimes the problem is caused by other shoulder conditions like prior fractures, arthritis, or instability. Irritation of the nerves that control the shoulder muscles is the culprit in about 5% of cases.
Although scapular dyskinesis can cause a variety of shoulder problems, it may initially go unnoticed. Up to 75% of healthy college athletes show some form of abnormal shoulder blade movement. If the condition is left untreated, you may begin to notice pain near the top of your shoulder. Sometimes the discomfort can radiate toward your neck or into your arm. Patients will often complain of a tender spot on the front of their shoulder. Long-standing altered mechanics can lead to bigger problems, including rotator cuff injury, shoulder instability, and arthritis.
The good news is that we have recognized the underlying cause of your shoulder problems and have treatments to correct it. You will need to perform your exercises consistently. You should also be conscious of your posture and try to avoid sitting or standing in “slouched” positions, as this is known to aggravate your problem.
Piriformis Syndrome; a real bummer.
Piriformis syndrome results from compression of the sciatic nerve as it passes underneath a muscle in your buttock called the piriformis. Your piriformis muscle attaches from the lowest part of your spine (sacrum) and travels across to your hip. The muscle helps to rotate your leg outward when it contracts. In most people, the sciatic nerve travels deep to the piriformis muscle.

When your piriformis muscle is irritated or goes into spasm, it may cause a painful compression of your sciatic nerve. Approximately ¼ of the population is more likely to suffer from piriformis syndrome because their sciatic nerve passes through the muscle.
Piriformis syndrome may begin suddenly as a result of an injury or may develop slowly from repeated irritation. Common causes include: a fall onto the buttocks, catching oneself from a “near fall,” strains, long distance walking, stair climbing or sitting on the edge of a hard surface or wallet. In many cases, a specific triggering event cannot be pinpointed. The condition is most common in 40-60 year olds and affects women more often than men.
Symptoms of piriformis syndrome include pain, numbness or tingling that begins in your buttock and radiates along the course of your sciatic nerve toward your foot. Symptoms often increase when you are sitting or standing in one position for longer than 15-20 minutes. Changing positions may help. You may notice that your symptoms increase when you walk, run, climb stairs, ride in a car, sit cross-legged or get up from a chair.
Sciatic arising from piriformis syndrome is one of the most treatable varieties and generally is relieved by the type of treatment provided in this office. You may need to temporarily limit activities that aggravate the piriformis muscle, including hill and stair climbing, walking on uneven surfaces, intense downhill running or twisting and throwing objects backwards, i.e., firewood. Be sure to avoid sitting on one foot and take frequent breaks from prolonged standing, sitting and car rides. You may find relief by applying an ice pack to your buttock for 15-20 minutes at a time, several times throughout the day.
Osteoporosis and Compression Fractures
Most of the tissues in our body are in a constant state of rejuvenation, wherein old cells are removed to be replaced by new. In our skeleton, when the production of new bone cannot keep up with the rate of tear down, our bones become progressively thinner and weaker in a process called “osteoporosis”.

Bone fractures occur when stress to a bone exceeds the bone’s ability to support that load. In healthy vertebrae, significant stress is required to cause a fracture. But in osteoporotic bones, the threshold for injury is lowered to the point that “compression fractures” may occur with seemingly minimal stress like bending, coughing, or sneezing. A compression fracture causes a wedge-shaped collapse of the front of the vertebral “body”- resembling what would occur after stepping on one edge of an aluminum can.
Compression fractures are two to three times more common in women, and the risk of developing the problem increases over time. People who have had a prior compression fracture are at greater risk for developing a subsequent fracture. Additional risk factors for compression fracture include a family history of osteoporosis, low body weight, recent weight loss, smoking, a sedentary lifestyle, poor dietary choices, inadequate calcium or vitamin D intake, excessive alcohol or caffeine intake, and scoliosis. The American Academy of Orthopedic Surgery recommends bone density screening for osteoporosis in all women over age 65 or post-menopausal women who have suffered a compression fracture. If you have not already done so, you should schedule a bone density screening.
Symptoms of a compression fracture include an “aching” or “stabbing” pain in the back, near the site of fracture. Symptoms can range from minimal to disabling. Often times, pain is referred to the ribs, hip, groin, or buttocks. Be sure to tell your doctor if you have pain or numbness that radiates into your legs, weakness, clumsiness, loss of bowel or bladder control, impotence, fever, unexplained weight loss, night sweats, excessive fatigue, or a history of cancer.
Symptoms from a compression fracture typically lasts for six to 12 weeks. Occasionally, patients will require surgical treatment of a compression fracture, but fortunately, most respond to conservative care. In general, you should maintain a relatively active lifestyle and try to avoid bed rest. If your pain prevents movement, you may talk to your doctor about wearing a brace to limit stress.
Our office will prescribe exercises to help you recover and reduce the risk of subsequent fracture. As your symptoms improve, you can begin incorporating some aerobic exercise, like walking on a treadmill. Studies have shown that light resistance training (i.e. weights and elastic bands) may help you maintain bone density and reduce the risk of future fractures. Supplements to help manage osteoporosis include daily intake of 800-1000 IU of vitamin D and 1000-1200 mg of calcium.
Did you know that you can breathe “wrong”?
Your “diaphragm” is the dome shaped muscle beneath your lungs. When it contracts and flattens, you breathe in. When it relaxes, you breathe out. But do you know your diaphragm plays an important secondary role in protecting your trunk and spine by controlling abdominal pressure?
The muscles that support your trunk form a “canister.” The front and sides of the canister are created by your abdominal and rib muscles. The back of the canister includes those muscles attached to your spine. The bottom of the canister is formed by the muscles of your pelvic floor, while your diaphragm serves as the roof. Together, these muscles control your abdominal pressure and core stability.

A well-braced core provides a stable foundation for moving your arms, legs, and head – in much the same way that when firing a canon, a large ship serves as a better platform than a rowboat.
During normal breathing, your upper chest should remain relatively still. Patients with “dysfunctional” patterns frequently overuse their upper chest muscles instead of their abdomen and lower rib cage. This depressurizes and destabilizes your core, leading to other problems like back pain.
You should not need to always think about proper breathing – this should happen subconsciously. Unfortunately, many of us have “learned” poor mechanics and need to re-learn proper breathing. One of the easiest ways to re-train proper breathing is to sit or lie still with one head on your breastbone and the other hand on your abdomen. When you breathe in, only the hand on your abdomen should move, while the hand on your chest remains still. Your normal breathing rhythm should be about there seconds of inhalation followed by six seconds of exhalation. If you find that you are exhaling too quickly, you may try “pursing” your lips to gradually increase the length of your exhalation.
The exercises that follow are essential for your recovery. Once you have restored normal breathing mechanics, you will enjoy increased core stability and your treatment will be much more successful. It is important to perform your breathing exercises consistently, as repetitive exercise will allow your body “re-learn” to subconsciously move in a safe and a coordinated fashion- thereby reducing your risk of injury.
Trigger points in the gluteus minimus
The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Lower Crossed Syndrome

Your posture plays an important role in your overall health. Poor posture leads to chronic strain and discomfort. “Lower crossed syndrome” is poor posture that results from excessive tightness in your lower back and hip flexor muscles with weakness in your abdominal and buttock muscles. Patients with lower crossed syndrome often have a “sway back.” Patients who sit for prolonged periods of time are at greater risk of lower crossed syndrome.
This postural problem commonly leads to painful conditions involving the back or hips. Successful treatment of lower cross syndrome involves stretching excessively tight muscles, strengthening weak muscles, taking frequent breaks from sitting, and modifying your workstation to be more user friendly.
Osgood Schlatter’s Disease
Children and adolescents have soft “growth plates,” which are areas where their bone is still growing. In children, this growth plate is much weaker than in adults. This means that children are more likely to suffer growth plate injuries than adults, especially during periods of rapid growth.
Osgood Schlatter’s disease, also called tibial epiphysitis, is a painful irritation of the growth plate near the insertion of your quadriceps muscle on your knee. The powerful thigh muscles attach onto your knee through the patellar tendon. When your thigh muscle contracts- like during running or jumping, they place a sheer force on the growth plate of your knee.
 Osgood Schlatter’s disease is more common in athletes, particularly those who participate in soccer, gymnastics, basketball, running or track. It is most common between the ages of 10 and 15 and is relatively equally common between boys and girls. Excessively tight thigh or calf muscles may contribute to this problem.
Osgood Schlatter’s disease is more common in athletes, particularly those who participate in soccer, gymnastics, basketball, running or track. It is most common between the ages of 10 and 15 and is relatively equally common between boys and girls. Excessively tight thigh or calf muscles may contribute to this problem.
You may experience pain with activity that requires running or jumping. You will often feel tenderness or even bony enlargement of your “tibial tuberosity”, just below your knee. Kneeling or prolonged squatting may be painful.
Some athletes with mild cases may continue activity as long as it does not increase your symptoms. Most cases may require a period of rest to allow the condition to heal. Depending on the severity of your condition, you may need to limit activities that require running and jumping for a while, usually two to eight weeks. You can often cross train in the pool or on a stationary bike.
You should avoid running with a narrow stride “on a line,” as this may increase your symptoms. Our office may recommend use of a patellar tendon strap to assist with your healing. Osgood Schlatter’s disease can temporarily limit your activity, but most of the time, it can be successfully managed, allowing your return to pain-free activity in a relatively short period of time.
Foot Over Pronation

The normal walking or running cycle begins with your heel striking the ground. As you transfer your body weight onto the front part of your foot, the arch of your foot naturally flattens slightly. This is called pronation.
The tissues that help maintain the arch of your foot are exposed to tremendous stress and may eventually break down. The loss of the normal arch of your foot results in a condition called “overpronation” or flat feet. This condition most commonly develops over a long period of time from repetitive stress.
Overpronation by itself is not painful, but the problem often leads to secondary problems, which may be painful. Plantar fasciitis, foot pain, shin splints and problems in the knee, hip or lower back are all related to overpronation. Patients who carry excess weight are more likely to develop this condition.
To help support your foot, you should wear shoes with good arch supports consistently. In some cases, specially molded orthotics may be needed to help support your arch.
What Is Upper Crossed Syndrome?
Your posture plays an important role in your overall health. Poor posture leads to chronic strain and discomfort. “Upper crossed syndrome” describes poor posture that results from excessive tightness in your shoulders and chest with weakness in your neck and mid-back. This combination forces your shoulders to roll inward and your head to project forward.

To help understand how upper crossed syndrome causes trouble, think of your spine as a telephone pole and your head as a bowling ball that sits on top. When the bowling ball is positioned directly over the top of the upright post, very little effort is required to keep it in place. If you tip the post forward and the ball begins to roll over the edge of the post, significantly more effort would be required from the muscles trying to hold it there. This effort results in chronic strain of the muscles of your neck and upper back.
The chronic strain is uncomfortable and may also lead to neck pain, upper back pain, headaches, TMJ pain, and ultimately- arthritis. This postural problem is exceptionally common in computer workstation users. Correction of this problem is accomplished by stretching the tight muscles, strengthening weak muscles, and modifying your workstation.
