The quadratus lumborum muscle is a commonly overlooked source of low back pain and is often responsible for “pseudo disc syndrome”. This muscle originates on the inferior border of the 12th rib and lumbar transverse processes. It inserts on the iliac crest and iliolumbar ligament. The q.l.’s main actions are extension and lateral flexion of the spine. It also acts as a stabilizer of the lumbar spine. Trigger points in this muscle refer pain into the sacroiliac joint and the lower buttock. Pain can also spread anteriorly along the crest of the ilium into the lower abdomen and groin and to the greater trochanter. 
Car Accident
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.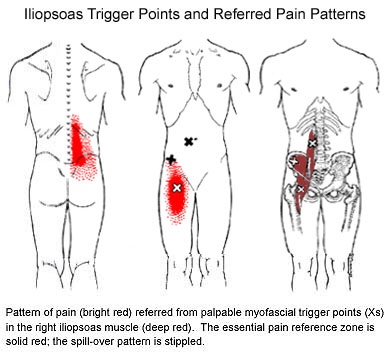
Can Chiro help me?

Chiropractic is the most widely accepted and most frequently used type of “alternative” healthcare in the United States. This is largely due to the fact that it works, and because of that, there has been a steady increase in acceptance by the public, third-party payers, and the Federal government. Since the mid-1990s, a number of outside (non-chiropractic) observers have suggested that chiropractic has now entered mainstream healthcare.
One can position chiropractic as being BOTH alternative and mainstream. It is “alternative” since it approaches healthcare from an entirely different direction compared to the primary care medical profession. Chiropractic is non-surgical and promotes diet and nutritional approaches vs. drugs and surgery. Chiropractic is also arguably “mainstream” as it has evolved into a strongly utilized form of primary care through popular acceptance and utilization by the public.
So, what role does chiropractic play in today’s health delivery system? This question is still being debated, but there appears to be three camps: 1) Specialist—limited to musculoskeletal (MSK) complaints on an interdisciplinary primary healthcare team; 2) Primary healthcare “gatekeepers” that focus on ambulatory MSK complaints; 3) Generalist primary healthcare provider of “alternative or complementary” medicine that manage and/or co-manage both MSK AND non-MSK conditions.
Looking at this from the patient or “consumer” perspective, chiropractic already plays an important role in the healthcare delivery for many patients. In 1993, a report claimed 7% of American adults had received chiropractic care during the prior year. According to a 2015 Gallup poll (that included 5,442 adults, aged 18+, surveyed between 2/16/15 and 5/6/15) entitled, Majority in U.S. Say Chiropractic Works for Neck, Back Pain, “Chiropractic care has a positive reputation among many US adults for effective treatment of neck and back pain, with about six in 10 adults either strongly agreeing (23%) or agreeing somewhat (38%) that chiropractors are effective at treating these types of pain.”
The “highlights” from this Gallup poll include: 1) Two-thirds say chiropractic is effective for neck and back pain. 2) Many adults say chiropractors think of the patient’s best interest. 3) More than 33 million adults in the United States (US) saw a chiropractor in the twelve months before the survey was conducted. That means roughly 14% of U.S. adults saw a chiropractor in the 12 months prior to the survey (vs. 7% in 1993). An additional 12% who responded to the Gallup pollsters saw a chiropractor in the last five years but not in the last 12 months. Overall, 51% of those polled had previously seen a chiropractor.
Whether or not you have personally utilized chiropractic, the educational process, licensing requirements, public interest, third-party payer systems, and interprofessional cooperation ALL support firm ground for which you can comfortably and confidently seek chiropractic care for your complaints.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care, we would be honored to render our services.
Where should you turn when back pain strikes?

Where should you turn when back pain strikes?
https://tribunecontentagency.com/article/where-to-turn-for-low-back-pain-relief/
Chiropractic should be a first line defence when back pain strikes. We are special trained to recognize the cause of back pain and treat when appropriate. When the cause is outside the scope of our practice, we are able to educate you on where you should go next.
Is there an actual cure all?

No; but exercise seems to be as close as we will ever get!
Some of you may have heard about how a modified form of boxing is helping patients with Parkinson’s disease (PD). If you haven’t, it’s been observed that people with Parkinson’s disease (PD) who engage in this boxing-like exercise routine can enhance their quality of life and even build impressive gains in posture, strength, flexibility, and speed. Proponents of the program report that regardless the degree of severity of PD, participants have a happier, healthier, and higher quality of life.
But must it be boxing? Maybe not. A report presented at the International Congress of Parkinson’s Disease and Movement Disorders in San Diego in June 2015 found that patients with Parkinson’s disease who began regular exercise early into the PD process had a much slower decline in their quality of life when compared with those who started exercising later. The researchers found just 2.5 hours per week of exercise is needed to improve quality of life scores. According to the report, it didn’t matter what exercise the participants did — simply getting up and moving for a total of 2.5 hours/week was reportedly enough (that’s only 20-25 minutes / day)!
Looking beyond Parkinson’s, other chronic conditions also benefit from adding exercise into a person’s lifestyle. Studies show that regular exercise as simple as walking helps reduce one’s risk for memory loss, and it slows down functional decline in the elderly. Incorporating aerobic exercise into one’s lifestyle can also improve reaction time in people at ALL AGES. Exercise has also been shown to improve both physical and emotional well-being in those afflicted with Alzheimer’s disease with as little as 60 minutes/week of moderate exercise! Patients with multiple sclerosis (MS) have also reported less stiffness and less muscle wasting when using exercise machines, aquatic exercise, and/or walking.
Research has shown just 30 minutes of brisk exercise three times a week can help reduce depressive symptoms in patients with mild-to-moderate depression. In a study involving teenagers, those who engaged in sports reported a greater level of well-being than their sedentary peers, and the more vigorous the exercise, the better their emotion health! In kids 8-12 years old, physical inactivity is strongly linked to depression.
Even anxiety, stress, and depression associated with menopause are less severe in those who exercise! So LET’S ALL GET OUT THERE AND EXERCISE!!!
My knee hurts; I must have bad knees….

Due to bipedal locomotion (walking around on two legs), foot and ankle problems have the potential to affect EVERYTHING above the feet—even the knees!
When analyzing the way we walk (also known as our gait), we find when the heel strike takes place, the heel and foot motion causes “supination” or the rolling OUT of the ankle. As the unloaded leg begins to swing forwards, there is a quick transition to pronation where the heel and ankle roll inwards and the medial longitudinal arch (MLA) of the foot flattens and pronates NORMALLY!
During the transition from supination to pronation, the flattening of the MLA acts like a spring to propel us forwards followed by the “toe off”, the last phase, as we push off with our big toe and the cycle starts with the other leg. However, if you watch people walk from behind, you will see MANY ankles roll inwards too much. This is call “hyperpronation” and that is NOT NORMAL!
So at what point does this normal pronation become hyperpronation? The answer is NOT black and white, as there is no specific “cut-off” point but rather, a range of abnormal. Hence, we use the terms mild, moderate, and severe hyperpronation to describe the variance or the degrees of abnormality. Hyperpronation can lead to the development of bunions and foot/ankle instability that can cause and/or contribute to knee, hip, pelvis, and spinal problems—even neck and head complaints can result (the “domino effect”)!
One study looked at the incidence of hyperpronation in 50 subjects who had an anterior cruciate ligament (ACL) rupture vs. 50 without a history of knee / ACL injury. They found the ACL-injured subjects had greater pronation than the noninjured subjects suggesting that the presence of hyperpronation increases the risk of ACL injury.
Doctors of chiropractic are trained to evaluate and treat knee conditions of all kinds. Often this may include prescribing exercises or utilizing foot orthotics in an effort to restore the biomechanics of the foot, which can have positive effects not only on the knees but also further up the body.
Pathophysiology of trigger points.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
Diagnosis of trigger points.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
Do I have a cuff tear?
One of the most common causes of shoulder pain is a rotator cuff (RC) tear. To determine just how common this is, one study looked at a population of 683 people regardless of whether or not they had shoulder complaints. There were 229 males and 454 females for a total of 1,366 shoulders. (The participants’ average age was 58 years, ranging from 22 to 87 years old.)
The research team found 20.7% had full thickness rotator cuff tears. Of those with shoulder pain, only 36% had tears found on ultrasound. Of those without shoulder pain, 17% also had tears! Risk factors for an increased for tearing of the rotator cuff include a history of trauma, the dominant arm (ie your right arm if you’re right handed), and increasing age.
In a review of radiologic studies of 2,553 shoulders, researchers found full-thickness rotator cuff tears in 11.75% and partial thickness tears in 18.49% of the subjects for a total of 30.24% having some degree of tearing. In this group, about 40% of tears were found in pain-free shoulders. The researchers concluded that rotator cuff tears are common and frequently asymptomatic.
Both of these studies support the necessity to FIRST consider the patient’s clinical presentation and then correlate that with the imaging results. In other words, the presence of a RC tear on an image (usually MRI or ultrasound) does NOT necessarily mean there is pain (and vise versa)!
So what other things could be causing the shoulder pain? There are many: impingement, tendonitis, bursitis, muscle strain, capsular (and other ligament) sprain, frozen shoulder, and osteoarthritis (the “wearing out” type). Also, rheumatoid arthritis, lupus, polymyalgia rheumatica and other autoimmune types of “arthropathies,” fibromyalgia, a herniated cervical disk, shoulder dislocations, whiplash injuries, and more!
Most importantly, we must NOT forget to include referred pain to the shoulder from an impaired heart (such as coronary heart disease or heart attack), lung, liver, or gall bladder as these problems commonly refer pain to the shoulder and may represent a MEDICAL EMERGENCY!
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
