The Lateral Pterygoid muscle is a muscle of the jaw. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate. It has its insertion on the condyloid process of the mandible. Functionally it it assists in opening the jaw by pulling the head of the mandibular condyle out of the mandibular fossa. Trigger points in this muscle refer pain into the temporal mandibular joint and maxillary sinus. Trigger points in this muscle are often the cause of pain felt from TMJ dysfunction.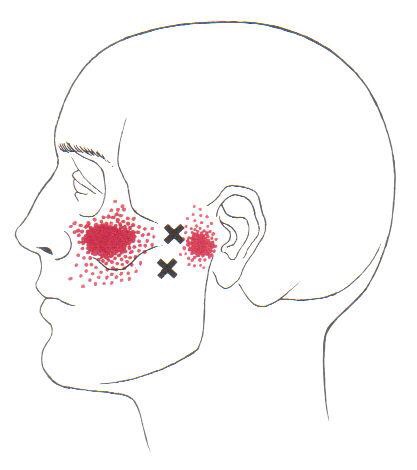
Car Accident
A treatment with Bryan Cobb RMT.
Session Description
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.
The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
What the Heck Is a Trigger Point?
By Bryan Cobb, Advanced Remedial Massage Therapist
What is a Trigger Point?
Trigger Points (TP’s) are defined as a “hyper-irritable spot within a taut band of skeletal muscle. The spot is painful on compression and can evoke characteristic referred pain and autonomic phenomena.”1
Put into plain language, a TP is a painful knot in muscle tissue that can refer pain to other areas of the body. You have probably felt the characteristic achy pain and stiffness that TP’s produce, at some time in your life.
TP’s were first brought to the attention of the medical world by Dr. Janet G. Travell. Dr. Travell, physician to President John F. Kennedy, is the acknowledged Mother of Myofascial Trigger Points. In fact, “Trigger Point massage, the most effective modality used by massage therapists for the relief of pain, is based almost entirely on Dr. Travell’s insights.”2 Dr. Travell’s partner in her research was Dr. David G. Simons, a research scientist and aerospace physician.
Trigger Points are very common. In fact, Travell and Simons state that TP’s are responsible for, or associated with, 75% of pain complaints or conditions.1 With this kind of prevalence, it’s no wonder that TP’s are often referred to as the “scourge of mankind”.
Trigger Points can produce a wide variety of pain complaints. Some of the most common are migraine headaches, back pain, and pain and tingling into the extremities. They are usually responsible for most cases of achy deep pain that is hard to localize.
A TP will refer pain in a predictable pattern, based on its location in a given muscle. Also, since these spots are bundles of contracted muscle fibres, they can cause stiffness and a decreased range of motion. Chronic conditions with many TP’s can also cause general fatigue and malaise, as well as muscle weakness.
Trigger Points are remarkably easy to get, but the most common causes are
•
TP’s (black dots) can refer pain to other areas (red)

Sudden overload of a muscle
• Poor posture
• Chronic frozen posture (e.g., from a desk job), and
• Repetitive strain
Once in place, a TP can remain there for the remainder of your life unless an intervention takes place.
Trigger Points Not Well Known
With thousands of people dealing with chronic pain, and with TP’s being responsible for — or associated with — a high percentage of chronic pain, it is very disappointing to find that a large portion of doctors and other health care practitioners don’t know about TP’s and their symptoms.
Scientific research on TP’s dates back to the 1700’s. There are numerous medical texts and papers written on the subject.
But, it still has been largely overlooked by the health care field. This has led to needless frustration and suffering, as well as thousands of lost work hours and a poorer quality of life.
How Are Trigger Points Treated?
As nasty and troublesome as TP’s are, the treatment for them is surely straight-forward. A skilled practitioner will assess the individual’s pain complaint to determine the most likely location of the TP’s and then apply one of several therapeutic modalities, the most effective of which is a massage technique called “ischemic compression”.
Basically, the therapist will apply a firm, steady pressure to the TP, strong enough to reproduce the symptoms. The pressure will remain until the tissue softens and then the pressure will increase appropriately until the next barrier is felt. This pressure is continued until the referral pain has subsided and the TP is released. (Note: a full release of TP’s could take several sessions.)
Other effective modalities include dry needling (needle placed into the belly of the TP) or wet needling (injection into the TP). The use of moist heat and stretching prove effective, as well. The best practitioners for TP release are Massage Therapists, Physiotherapists, and Athletic Therapists. An educated individual can also apply ischemic compression to themselves, but should start out seeing one of the above therapists to become familiar with
the modality and how to apply pressure safely.
1 Simons, D.G., Travell, D.G., & Simons, L.S. Travell and Simons’ Myofascial Pain and Dysfunction: the Trigger Point Manual.
Vol. 1. 2nd ed. Lippincott, Williams, and Wilkins, 1999.
2http://www.muscletherapyworks.com/MTW%20Biography%20T%20&%20S%2001.htm
Trigger points in the deltoid muscle
The deltoid is the main muscle that makes up the shoulder. It originates on the clavicle, acromion, and spine of the scapula. It inserts on the deltoid tuberosity of the humerus. The deltoid acts at the shoulder to produce abduction, and assist with flexion and extension. The deltoid is especially prone to developing trigger points. These posterior style will refer pain into the anterior and lateral shoulder. Trigger points in the posterior delt will refer pain into the posterior shoulder with spillover down the lateral arm.
Lumbar Radiculopathy? That sounds ridiculous!
Your nervous system is basically a big electrical circuit. Your spinal cord transmits all of the electrical nerve impulses between your brain and lower back. From there, individual nerves emerge from your spine then travel to supply sensation and movement to a specific area of your buttock, legs and/or feet. This allows you to move and feel sensations like touch, heat, cold and pain. Anything that

interferes with this transmission can cause problems.
You have been diagnosed with a “Lumbar Radiculopathy”. This means that one or more of the nerves emerging from your lower back has become irritated or possibly pinched. This often results in pain, numbness or tingling in the specific area of your leg that is supplied by the irritated nerve. The term “Sciatica” is often used to describe this condition, because most (but not all) “lumbar radiculopathies” involve the sciatic nerve which supplies the back & outside of your thigh and calf. Symptoms of a lumbar radiculopathy may vary from a dull ache to a constant severe sharp shooting pain. Your symptoms are likely aggravated by certain positions or movements.
To solve this problem, we will treat the source of your nerve irritation. It is important for you to follow your treatment plan closely and be sure to tell us immediately if you experience any progression of your leg pain, numbness or weakness.
Lumbar Spondylolisthesis
Your spine is made up of 24 individual vertebrae all stacked on top of each other. The lowest five vertebrae are referred to as your lumbar spine. Each vertebra has two basic components: the “body” and the “arch.” You can envision this as a coffee mug lying on its side. The cup would represent the vertebral body, and the handle would represent the arch. The spinal cord travels through each of


the vertebral arches on its way from your brain to your tailbone. The term “lumbar isthmic spondylolisthesis” describes a condition where your arch has broken free from its anchor on the vertebral body, allowing the vertebral body to slide forward. Lumbar spondylolisthesis typically affects the lowest lumbar vertebra, L5, or occasionally the second lowest, L4.
The condition is sometimes caused by trauma, but more often follows a “stress fracture” involving the arch of the vertebra. This break and slippage is thought to result from repetitive movements, especially hyperextension (arching back) and rotation. The break usually happens during childhood but does not always cause symptoms when it occurs. Many times, the condition will lie dormant until later in life. Lumbar spondylolisthesis is present in six to seven percent of the population and affects males twice as often as females. The problem is more common in those who participate in sports. Some sports predispose children to this “break and slip”. Athletes who participate in gymnastics, rowing, diving, football, wrestling, weight lifting, swimming, tennis, volleyball, and track & field throwing sports (i.e. discus, shot put, etc) are at greatest risk.
The pain usually starts in your back but may radiate into your buttock or thigh. Your pain usually intensifies with standing upright for prolonged periods of time or leaning backwards, especially during heavy activity. Some women report increased symptoms during the later stages of pregnancy. Be sure to tell your doctor if you notice pain, numbness or tingling in your groin, a loss of bowel or bladder function, fever, night sweats, pain extending beyond your knee, or weakness in your legs.
Your doctor will “grade” your spondylolisthesis based on the percent of the vertebral body that has slipped forward. Your doctor will try to determine if your spondylolisthesis is “active”, meaning a recent break or “inactive”, referring to a long-standing problem. If your doctor has determined that your spondylolisthesis is new and has a chance of worsening, you may need to stop certain activities or sports for a period of time until your fracture heals. Sometimes a lumbar brace is used to help you recover more quickly. Patients with a long-standing “inactive” spondylolisthesis may benefit from a combination of treatments including stretching and strengthening. You should limit leaning backwards or sleeping on your stomach. Females should avoid wearing high heels.
Positive Expectations in Whiplash Patients Help with Recovery

“High expectations are the key to everything”
– Sam Walton
Now a new study found that this belief may apply to your health as well: Whiplash patients who have a positive expectation to improve tend to recover better and report less pain than those who harbor negative beliefs like fearing movement and re-injury.
If you or someone you know has been involved in accident, call our office today. Check out THIS VIDEO to learn more about resolving neck pain from auto accidents.
Ouch! My Back Went Out!
Your spine consists of 24 individual vertebrae stacked on top of each other. Flexible cushions called “discs” live between each set of vertebrae. A disc is made up of two basic components. The inner disc, called the “nucleus”, is like a ball of jelly about the size of a marble. This jelly is held in place by the outer part of the disc called the “annulus”, which is wrapped around the inner nucleus much like a ribbon wrapping around your finger. The term lumbar disc lesion means that your disc has been damaged.


Disc lesions start when the outer fibers of the disc become strained or frayed. If enough fibers become frayed, this can create a weakness and when the disc is compressed, the outer fibers may “bulge” or “protrude” like a weak spot on an inner tube. If more fibers are damaged, the nucleus of the disc may “herniate” outward. Since the spinal cord and nerve roots live directly behind the disc, bulges that are accompanied by inflammation will likely create lower back pain that radiates into the buttock or the entire lower extremity. This condition is called sciatica. If the disc bulge is significant enough to create a mechanical compression of your nerve, you may also experience loss of your reflexes and weakness. Be sure to let our office know if you notice progressive weakness or numbness, any numbness around your groin, any loss of bowel or bladder control or fever.
Surprisingly, disc bulges are present without any symptoms in about 1/3 of the adult population. Another one third of adults will experience pain from a lumbar disc at some point in their lifetime. The condition is more common in men. Most lumbar disc problems occur at one of the two lowest discs- L5 or L4. Smokers and people who are generally inactive have a higher risk of lumbar disc problems. Certain occupations may place you at a greater risk, especially if you spend extended periods of time sitting or driving. People who are tall or overweight have increased risk of disc problems. The condition is uncommon in children and is most common between the ages of 40 and 60.
Researches have shown that disc bulges and sciatica may be successfully managed with conservative care like the type we will provide.
Trigger points in the adductor longus and brevis.
These muscles are located in the groin. The longus originates on the pubic body just below the pubic crest and inserts on the middle third of the linea aspera.The brevis muscle originates on the inferior ramus and body of the pubis and has its attachment to the lesser trochanter and linea aspera of the femur. Trigger points in these muscles are the most common muscular cause of groin pain. Distal trigger points refer pain to the upper medial knee and down the tibia. Proximal trigger points refer into the anterior hip area.
Bryan Cobb RMT.
Since 2005, Bryan has been dedicated to helping all people with chronic and acute pain caused by soft-tissue damage.
His training and experience make him uniquely qualified to treat a wide variety of pain and dysfunction and to give instruction on prevention and self-care.
Bryan is the only Massage Therapist in Manitoba — and one of the few in Canada — to be certified by the Certification Board for Myofascial Trigger Point Therapists (CBMTPT).
Bryan holds a degree as an Advanced Remedial Massage Therapist (ARMT) from the Massage Therapy College of Manitoba. Course work at MTCM includes
• over 2,000 hours of practice, as well as
• intensive course work,
• a supervised clinical practicum, and
• community outreach placements.MTCM has a credit transfer affiliation with the University of Winnipeg, ensuring that its courses are held to the highest level. When Bryan studied at MTCM, the college was the only massage therapy college in western Canada accredited by the Commission on Massage Therapy Accreditation. Today, the college is a member of the Canadian Council of Massage Therapy Schools.
Bryan is a member in good standing of the Natural Health Practitioners of Canada.
Bryan also has a background in Anatomy, Exercise Physiology, and Sport Sciences from the University of Manitoba, and he has worked as a personal trainer and fitness leader.
He is an avid natural bodybuilder and fitness enthusiast, and has a blue belt in Brazilian jiu-jitsu.
Suddenly my back was killing me!
Low back pain affects 80% of the population at some point in their life and one-third of the population on a yearly basis. One of the most common causes of low back pain comes from a slightly restricted joint in your spine.
 Your lower back is made up of 5 bones stacked on top of each other with a soft “disc” between each segment to allow for flexibility. Normally, each joint in your spine should move freely and independently. Our examination of your spine has shown that one or more of the joints in your low back is slightly misaligned and restricted. We call this condition “lumbar segmental joint restriction”.
Your lower back is made up of 5 bones stacked on top of each other with a soft “disc” between each segment to allow for flexibility. Normally, each joint in your spine should move freely and independently. Our examination of your spine has shown that one or more of the joints in your low back is slightly misaligned and restricted. We call this condition “lumbar segmental joint restriction”.
To help visualize this, imagine a normal spine functioning like a big spring moving freely in every direction. A spine with a joint restriction is like having a section of that spring welded together. The spring may still move as a whole, but a portion of it is no longer functioning.
Joint restriction can develop in many ways. Sometimes they are brought on by an accident or an injury. Other times, they develop from repetitive strains or poor posture. Several factors may make you more likely to experience low back problems. These include: being overweight, smoking, strenuous work, repetitive bending, twisting and lifting, prolonged exposure to whole body vibration- i.e. operating a motorized vehicle, stress, anxiety, depression, dissatisfaction with your job and even your attitude!
Restricted joints give rise to a self-perpetuating cycle of discomfort. Joint restriction causes swelling and inflammation, which triggers muscular guarding leading to more restriction. Since your spine functions as a unit, rather than as isolated pieces, a joint restriction in one area of your spine often causes “compensatory” problems in another. Think of this as a rowboat with multiple oarsmen on each side. When one rower quits, the others are placed under additional stress and can become overworked.
Joint restrictions most commonly cause local tenderness and discomfort. You may notice that your range of motion is limited. Movement may increase your discomfort. Pain from a restricted joint often trickles down to your hips or thighs. Be sure to tell your chiropractor if your symptoms include any radiation of pain below your knee, weakness, groin numbness or changes in bowel or bladder function.
Long-standing restrictions are thought to result in arthritis – much like the way a slightly misaligned wheel on your car causes premature wearing of your tire.
You should recognize that your problem is common and generally treatable. Chiropractic care has been shown to be the safest and most effective treatment for joint restrictions. Our office offers several tools to help ease your pain. To speed your recovery, you should wear supportive shoes and avoid activities that increase your pain. Be sure to take frequent breaks from sedentary activity. Yoga has been shown to help back pain sufferers so consider joining a class or picking up a DVD.
