Thoracic Outlet Syndrome (TOS)
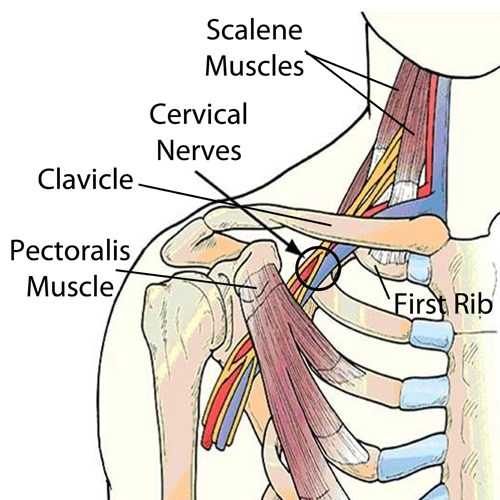
The term “thoracic outlet” describes an area at the base of your neck, just above your collarbone. Some important nerves and vessels pass through this outlet on their way into your arm. Compression of these tissues causes a condition called “thoracic outlet syndrome” which results in pain, numbness or tingling in your arm.
Several different factors can cause Thoracic Outlet Syndrome, commonly referred to as TOS. Sometimes TOS is caused from tightness in the muscles of your neck and chest, other times the space between your first rib and collarbone is too small. People who have an extra rib (cervical rib) and people who have recently suffered a neck injury may have a greater chance of having this problem.
The condition is aggravated by poor posture and by occupations that promote “slouching,” i.e., computer users, assembly line workers, supermarket checkers and students. Swimmers, volleyball players, tennis players, baseball pitchers and occupations requiring prolonged overhead activity. i.e., electricians and painters are also prime candidates for TOS.
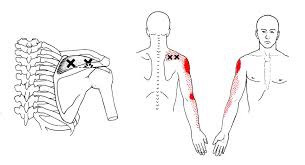
Symptoms of TOS include arm pain, numbness, tingling and possible weakness. Neck, arm and hand pain may begin slowly and are often aggravated by elevation of the arms or excessive head movement. Loss of grip strength is possible.
Conservative treatment, like the kind we provide, has been shown to be effective at treating TOS. Through our careful exam we have identified your specific sites of compression and will use some of the following treatment to help:
You should avoid carrying heavy loads, especially on your shoulder i.e., carpet rolls. Briefcases, laptop cases or heavy shoulder bags should be lightened. Bra straps may need additional padding or consideration of replacement with a sports bra.