The temporalis muscle is located in the temple area of the skull. It originates on the temporal lines on the parietal bone of the skull, and inserts on the coronoid process of the mandible. It’s main action is to close the jaw. The posterior and middle fibres bilaterally retrude the mandible. Acting individually, this muscle will deviate the mandible to the same side. Trigger points in this muscle refer into the teeth causing hypersensitivity, and into and above the eye and temple, causing headaches.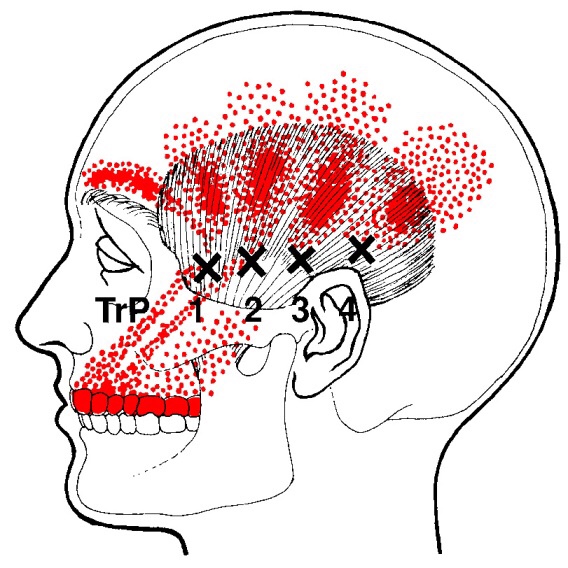
Aging
Osteoarthritis of the Hand
The bones in your hand have a slick, protective covering called “cartilage” on the joint surfaces that touch each other. This cartilage serves as a friction reducer and shock absorber, thereby, helping to extend the life of your joints. “Arthritis” means that your cartilage has begun to thin or crack and may eventually wear away –impairing your strength and dexterity. Painful hand arthritis affects

up to 1 in 4 people. This degeneration has a tendency to affect specific joints, especially those of your index and middle fingers and the base of your thumb.
Your chance of developing arthritis increases with age. Hand arthritis is 2 1/2 times more common in women. Arthritis occurs more often in joints that have been previously injured and in patients who perform repetitive movement of the hands- particularly labor and manufacturing jobs. Other risk factors include obesity and the presence of arthritis in your parents. Contrary to popular opinion, knuckle cracking does not increase your risk of arthritis, regardless of duration or frequency.
Symptoms usually begin slowly and progress into longstanding hand pain that comes and goes. Your symptoms are likely aggravated by activity and relieved by rest. Hard, bony enlargements often develop along the joint lines, especially in women. You may notice morning stiffness that subsides fairly quickly. Be sure to tell your doctor if you notice lasting morning stiffness or swelling, as this could be a sign of a different type of arthritis.
The American College of Rheumatology recommends the use of non-drug treatments (like the type provided in this office) for hand osteoarthritis. Patients with thumb osteoarthritis may benefit from a nighttime splint. Topical creams, especially those including “capsaicin” may help relieve symptoms. You may find relief by warming your hands with a hot pack or “paraffin bath” when they feel stiff. Some patients report benefit by taking Glucosamine Sulfate. The mainstay of treatment includes exercises to help improve your mobility and strength.
What is Tarsal Tunnel Syndrome?
The tarsal tunnel is the space behind the bump on the inside of your ankle. The tibial nerve lives in this tunnel along with some tendons. Tarsal tunnel syndrome means that the tibial nerve is being irritated within the tunnel. This results in pain, numbness or tingling into your heel and the arch of your foot.
The tibial nerve may be irritated by compression (from trauma , arthritic spurs, or swelling of other tissues within the tunnel), or more commonly by constant stretch (from flat feet). Research has shown that tarsal tunnel pressure increases almost 30 fold in people with flat feet.
 Tarsal tunnel is slightly more common in women, and high heels are suspect. The condition often affects both feet. Conditions like diabetes and thyroid disorders may aggravate nerve problems like tarsal tunnel. Plantar fasciitis commonly accompanies tarsal tunnel syndrome.
Tarsal tunnel is slightly more common in women, and high heels are suspect. The condition often affects both feet. Conditions like diabetes and thyroid disorders may aggravate nerve problems like tarsal tunnel. Plantar fasciitis commonly accompanies tarsal tunnel syndrome.
The discomfort is often described as “burning”. Symptoms may increase with long periods of standing, running or exercise. Almost half of patients report increased symptoms at night.
Your doctor will make the diagnosis of tarsal tunnel syndrome based on your history and an exam. Your doctor may take an x-ray to rule out other problems like arthritic spurs or a stress fracture. In severe cases, more sophisticated nerve testing may be necessary.
The first goal of treatment is to allow you to return to pain-free activity as soon as possible. The second goal is to correct the mechanical problem that allowed this condition to begin with.
Spring Cleaning Tips
If you plan on doing a bit of spring cleaning soon, here is our friendly safety reminder: Don’t forget that some chores are a workout, so stretch accordingly before and after. Also, be mindful of your posture throughout your cleaning.
Keep a neutral spine, bend at your knees when lifting heavy items, and never twist your back at unhealthy angles.
There is nothing great about greater trochanteric pain syndrome. Nothing at all.
Your hip typically has about six small fluid-filled sacs called “bursa” that act as cushions between tendons and bone. One of the most common causes of hip pain is a condition called, “hip bursitis” which means that one or more of your bursas have become painfully inflamed. The broader (more accurate) diagnosis of “Greater trochanteric pain syndrome” (GTPS) describes an uncomfortable collection of problems affecting the outermost portion of your hip. GTPS can include swelling of one or more of the fibrous tendons that attach your muscles onto your hip – a condition called, “tendinitis.” In addition to bursitis & tendonitis, GTPS may originate from tightness in the muscle that travels over your hip en route to your knee- resulting in compression and irritation to your hip.

Greater trochanteric pain syndrome is most common in middle age to elderly adults and is 2-4 times more common in females. Sometimes the problem affects both hips at the same time. Approximately 1/3 of patients with GTPS have lower back pain. Patients who have arthritis in their hips and knees are more likely to suffer from ongoing complaints.
Your symptoms probably include a persistent pain on the outside of your hip, buttock, and upper thigh. Your discomfort may be aggravated by sitting with your leg crossed, arising from a seated position, prolonged standing, climbing stairs, and high-impact activities, like running. Sometimes patients find it difficult to sleep, since lying on the painful hip usually increases symptoms.
For adults, x-rays may or may not be needed to confirm the diagnosis, but children and adolescents usually require films to rule out more serious childhood diseases. Be sure to tell your doctor if you notice that you have a fever, leg numbness, pain radiating significantly beyond your knee, or pain in the front of your groin crease (the area where you leg meets your pelvis.)
Conservative treatment, like the type provided in this office, is successful in about 90% of cases. If you have acute pain, you may need to temporarily limit or discontinue activities that increase your discomfort. Using ice or ice massage at home may help. Some patients find temporarily relief by applying sports creams. Very commonly, patients with pain on the outside of their hip suffer from weakness in one of their buttock muscles, called the “gluteus medius.” When this muscle lacks strength, it is unable to protect your hip during normal activities, like walking. Research has shown that strengthening your hip has a dramatic effect on your progress.
Athletes should avoid running on a banked surface, like the crown of a road or indoor track. Be sure to reverse directions each mile if you run on a circular track. Avoid running on wet or icy surfaces, as this can cause increased tension in your hip. Runners with a “lazy” narrow-based running gait will benefit by increasing their step width to minimize stress on their hip. Cyclists need to make sure that their seat is not positioned too high. Overweight patients should consider weight reduction programs.
Osteoporosis and Compression Fractures
Most of the tissues in our body are in a constant state of rejuvenation, wherein old cells are removed to be replaced by new. In our skeleton, when the production of new bone cannot keep up with the rate of tear down, our bones become progressively thinner and weaker in a process called “osteoporosis”.

Bone fractures occur when stress to a bone exceeds the bone’s ability to support that load. In healthy vertebrae, significant stress is required to cause a fracture. But in osteoporotic bones, the threshold for injury is lowered to the point that “compression fractures” may occur with seemingly minimal stress like bending, coughing, or sneezing. A compression fracture causes a wedge-shaped collapse of the front of the vertebral “body”- resembling what would occur after stepping on one edge of an aluminum can.
Compression fractures are two to three times more common in women, and the risk of developing the problem increases over time. People who have had a prior compression fracture are at greater risk for developing a subsequent fracture. Additional risk factors for compression fracture include a family history of osteoporosis, low body weight, recent weight loss, smoking, a sedentary lifestyle, poor dietary choices, inadequate calcium or vitamin D intake, excessive alcohol or caffeine intake, and scoliosis. The American Academy of Orthopedic Surgery recommends bone density screening for osteoporosis in all women over age 65 or post-menopausal women who have suffered a compression fracture. If you have not already done so, you should schedule a bone density screening.
Symptoms of a compression fracture include an “aching” or “stabbing” pain in the back, near the site of fracture. Symptoms can range from minimal to disabling. Often times, pain is referred to the ribs, hip, groin, or buttocks. Be sure to tell your doctor if you have pain or numbness that radiates into your legs, weakness, clumsiness, loss of bowel or bladder control, impotence, fever, unexplained weight loss, night sweats, excessive fatigue, or a history of cancer.
Symptoms from a compression fracture typically lasts for six to 12 weeks. Occasionally, patients will require surgical treatment of a compression fracture, but fortunately, most respond to conservative care. In general, you should maintain a relatively active lifestyle and try to avoid bed rest. If your pain prevents movement, you may talk to your doctor about wearing a brace to limit stress.
Our office will prescribe exercises to help you recover and reduce the risk of subsequent fracture. As your symptoms improve, you can begin incorporating some aerobic exercise, like walking on a treadmill. Studies have shown that light resistance training (i.e. weights and elastic bands) may help you maintain bone density and reduce the risk of future fractures. Supplements to help manage osteoporosis include daily intake of 800-1000 IU of vitamin D and 1000-1200 mg of calcium.
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
Some Sleep Habit Tips

Researchers recommend sleeping for 7-9 hours per night. Even small deficits can pose problems like decreased athleticism, diminished brain function, increased inflammation and a greater likelihood to get sick- sleeping only 6 hours per night makes you four times more likely to catch a cold when compared to sleeping 7 or more hours. Follow these additional tips for better sleep:
✓ Limit screen time before retiring- the blue light emitted from computer monitors, phones and TV’s can limit melatonin production and adversely affect sleep. Try reading from a book or magazine instead.
✓ Ideally, eat your last meal 3-4 hours before bedtime and especially limit heavy, spicy or high-fat foods. Ration how much you drink before bedtime to minimize bathroom breaks. Particularly limit caffeine in the afternoon and evening- caffeine has a half-life of 6-9 hours and can keep you awake long after the last sip.
✓ Stick to a sleep schedule, trying to retire and arise at the same time each day, including weekends.
✓ Sleep on a comfortable mattress and pillow. Choose 100% cotton sleep clothes and sheets over synthetic materials (i.e. polyester). Some research has suggested that your “deep” REM sleep improves when your mattress is oriented so that your body is aligned North and South as opposed to East and West.
✓ Most people sleep best in a cool room; ideally between 60-67 degrees F.
What is a trigger point
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
Snapping Hip. Not as horrific as it sounds.
The muscle responsible for flexing your hip toward your trunk, is called the Psoas. This muscle begins on your lower spine and passes through your pelvis to attach onto the top of your femur (thigh bone). Along this course, the muscle travels across the front of your hip socket and over several bony prominences. If the muscle is too tight, its tendon may rub over these “bumps”. This occasionally produces an audible snapping sound, hence the moniker, “snapping hip”, aka “psoas tendinopathy”.
 The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
The tendon can be irritated by an acute injury, but more commonly from overuse- particularly repeatedly flexing your hip toward your trunk. The condition is also known as “dancer’s hip” or “jumper’s hip”, as movements associated with these activities are known culprits. Likewise, the condition is frequently seen in athletes who participate in rowing, track and field, hurdling, running (especially uphill), soccer, and gymnastics.
Your symptoms may include a “snapping” sound or sensation when you flex and extend your hip- although many cases are silent. Repeated rubbing causes inflammation and subsequent deep groin pain that can radiate to the front of your hip or thigh. Long-standing problems can trigger weakness or even limping.
The diagnosis of snapping hip is frequently overlooked. In fact, some studies show that identification is often delayed more than two years, while other potential causes are pursued. Fortunately, your problem has been recognized, and our office has several treatments to help you recover.
Psoas problems often start when one group of muscles is too tight, while another is too loose. Your home exercises will help to correct this problem. Depending upon the severity of your condition, you may need to avoid certain activities for a while. You should especially avoid repetitive hip flexion. Prolonged seated positions can encourage shortening of your hip flexors so be sure to take frequent breaks. Patients with fallen arches may benefit from arch supports.
