Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
Whiplash
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
He barely hit me; why does it hurt?
Error
This video doesn’t exist
You may have heard the comment, “If there’s no damage to the car, then there’s no injury.” Unfortunately, that does not always seem to be the case.
There are MANY factors that affect the dynamics of a collision and whether or not injury occurs. A short list includes: vehicle type and design, speed, angle of collision, momentum, acceleration factors, friction, kinetic and potential energy, height, weight, muscle mass, seat back angle and spring, head position upon impact, etc.
Consider Sir Isaac Newton’s Third Law of Motion: “For every action there is an equal and opposite reaction.” This law applies to a car accident at any speed. Using the analogy of hitting a pool ball into the corner pocket straight on, when the cue ball stops, its momentum is transferred to the target ball which accelerates at the same speed…hopefully into the corner pocket!
This example is not quite the same as an automobile collision because the energy transfer is very efficient due in part to the two pool balls not deforming (crushing or breaking) on impact with one another. If either ball did deform, more energy absorption would occur and the acceleration of the second ball would be lower.
In fact, in the United States, vehicle bumpers are tested at 2.5 mph with impact equipment of similar mass with the test vehicle’s brakes disengaged and the transmission in neutral. National Highway Transportation Highway Safety Administration (NHTSA) vehicle safety standards demand that no damage should occur to the car in this scenario.
However, energy transfer occurs very quickly and with a greater amount of force when there is no vehicle deformation (damage). As a result, a greater amount of energy (described as G-force) is directly transferred to the occupants inside the vehicle—increasing the risk of injury. A 1997 Society of Automobile Engineers article provided an example in which the same 25 mph (12 m/s) collision resulted in a five-times greater force on the occupants of the vehicle when the crush distance of the impact fell from 1 meter to .2 meters.
So be aware that even low-speed impacts can still place quite a bit of force on your body, even if the bumper of your car doesn’t have a scratch on it.
What is a Migraine? What can I do about them?
A “migraine” is an intense throbbing headache that may be accompanied by nausea, vomiting, and sensitivity to light or noise. Adult women are three times more likely than men to experience migraines. The frequency of migraine headaches usually peaks between age 30 and 40, and attacks decrease thereafter. The onset of a new migraine headache after age 50 is rare.
 Migraine headaches are caused by a combination of nerve irritation and enlargement of the blood vessels in your brain. Migraines tend to run in families and sufferers have inherited a sensitive nervous system from their parents. Patients who are overweight or have other vascular risk factors are more likely to suffer from migraines.
Migraine headaches are caused by a combination of nerve irritation and enlargement of the blood vessels in your brain. Migraines tend to run in families and sufferers have inherited a sensitive nervous system from their parents. Patients who are overweight or have other vascular risk factors are more likely to suffer from migraines.
Migraines are set off by “triggers” and the headache occurs when the number of triggers reaches a critical threshold. This can be likened to a glass of water that overflows at a certain point. Known triggers include: neck tightness, stress, smoking, strong odors (i.e. perfumes), bright or flickering lights, fluorescent lighting, too little or much sleep, head trauma, weather changes, motion sickness, cold (ice cream headaches), lack of activity or exercise, overexertion, fatigue, eyestrain, dehydration, hunger, fasting, and hormonal changes, including menstruation and ovulation. Certain medications, including hormones or oral contraceptives are known triggers. A detailed list of foods that trigger migraines is provided below.
About 20-33% of people who get migraines have warning symptoms, called an “aura”, before their actual headache attack. Aura symptoms develop slowly over five to 20 minutes and can last up to an hour. The most common aura is a band of absent vision with an irregular shimmering border. Some patients report numbness or tingling in their arms or face. Be sure to tell your doctor if you experience any confusion or decreased consciousness with your headache. Other signs to watch for include: abrupt headaches that develop and peak very quickly, headaches that develop following a head injury, light-headedness, dizziness, difficulty speaking, difficulty swallowing, difficulty walking, fever, rash, or any “new” headache that is significantly different from your prior headaches.
Many patients benefit from the types of treatment provided in this office. Research has shown a “significant reduction” in migraine frequency and intensity through chiropractic care. Your home management will focus on avoiding “triggers” and stress. You should begin keeping a headache diary to help you track and eliminate triggers. Patients who experience migraines are more susceptible to other types of cardiovascular disease, like heart attack and stroke. Be sure to choose a “heart healthy” diet (i.e. limit sodium and fats) and keep your weight controlled. Eat at regular intervals and stay well-hydrated as hunger and dehydration are known triggers.
Your doctor may talk to you about supplements like Feverfew (125mg/ day), Riboflavin (400mg/ day), Magnesium (400-600mg/ day) and Co-enzyme Q10 (100mg 3x per day) that have been helpful in preventing headaches for some migraine sufferers. The American Headache Society recommends that patients avoid overuse of medication to control their headaches, (no more than 2 doses per day, 2 days/week) as this can lead to more frequent “rebound” headaches. Do not begin or discontinue any new vitamins or medications without talking to your doctor first, especially if you are nursing or pregnant.
Why am I so dizzy after my whiplash?

Whiplash, or better termed “Whiplash Associated Disorders” (WAD), is a condition that carries multiple signs and symptoms ranging from neck pain and stiffness to headache, confusion, ringing in the ears, and more. But can WAD cause dizziness? Let’s take a look!
Dizziness is a general term that is used rather loosely by the general population. We’ve all experienced dizziness from time-to-time that is considered “normal,” such as standing up too quickly or while experiencing a rough flight.
Often, dizziness and problems with balance go hand in hand. There are three main organs that control our balance: 1) the vestibular system (the inner ear); 2) the cerebellum (lies in the back of the head); and, 3) the dorsal columns (located in the back part of the spinal cord). In this article, we will primarily focus on the inner ear because, of the three, it’s unique for causing dizziness. Our vision also plays an important role in maintaining balance, as we tend to lose our balance much faster when we close our eyes.
It’s appropriate to first discuss the transient, usually short episode of “normal” lightheadedness associated with rising quickly. This is typically caused by a momentary drop in blood pressure, and hence, oxygen simply doesn’t reach the brain quick enough when moving from sitting to standing. Again, this is normal and termed “orthostatic hypotension” (OH).
However, OH can be exaggerated by colds, the flu, allergy flair-ups, when hyperventilating, or at times of increased stress or anxiety. OH is also associated with the use of tobacco, alcohol, and/or some medications. Bleeding can represent a more serious cause of OH such as with bleeding ulcers or some types of colitis, and less seriously, with menstruation.
The term BPPV or benign paroxysmal positional vertigo, has to do with the inner ear where our semicircular canals are located. The canals lie in three planes and give us a 3D, 360º perspective about where we are in space. The fluid flowing through these canals bends little hair-like projections, which are connected to sensory nerves that tell the brain about our spatial position. If the function of these canals is disturbed, it can mix-up the messages the brain receives, thus resulting in dizziness. Exercises are available on the Internet that can help with BPPV (look for Epley’s and Brandt-Daroff exercises).
DANGEROUS causes of dizziness include: HEART – fainting (passing out) accompanied by chest pain, shortness of breath, nausea, pain or pressure in the back, neck, jaw, upper belly, or in one or both arms, sudden weakness, and/or a fast or irregular heartbeat.
STROKE – sudden numbness, paralysis, or weakness in the face, arm, or leg, especially if only on one side of the body; drooling, slurred speech, short “black outs,” sudden visual changes, confusion/difficulty speaking, and/or a sudden and severe, “out of the ordinary” headache. CALL 911 (or the number for emergency services if you’re outside the Canada) if you suspect you may be having a heart attack or stroke!
Trigger points in the trapezius muscle.
The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
How long does Whiplash last?

First, what is whiplash? It’s a lot of things, which is why the term WAD or Whiplash Associated Disorders has become the most common term for the main signs and symptoms associated with a whiplash injury. WAD is usually associated with a motor vehicle collision, but sports injuries, diving accidents, and falls are other common ways to sustain a WAD injury.
To answer the question of the month, in most cases, the recovery rate is high and favors those who resume their normal daily activities. The worse thing you can do when you sustain a WAD injury is to not do anything! Too much rest and inactivity leads to long-term disability. Of course, this must be balanced with the degree of injury, but even when the injury requires some “down time,” stay as active as possible during the healing phase.
Many people recover within a few days or weeks while a smaller percentage require months and about 10% may only partially recover. So what can be done to give you the best possible chance to fully recover as soon as possible?
During recovery, you can expect your condition to fluctuate in intensity so “listen” to your body, let it “guide” you during activity and exercise, and stay within “a reasonable boundary of pain” during your activity. Remember, your best chance for full recovery FAVORS continuing a normal lifestyle. Make reasonable modifications so you can work, socialize, and do your “normal” activities!
The KEY: Stay in control of your condition – DO NOT let it control you! Here are some tips:
1) POSTURE CONTROL: Keep the weight of the head back by gliding your chin back until you “hit” a firm end-point. Then release it slightly so it’s comfortable—this is your NEW head position!
2) FLEXIBILITY: Try this range of motion (ROM) exercise… Slowly flex your neck forwards and then backwards, then bend your neck to the left and then the right, and then rotate it to the left and to then to the right. THINK about each motion and avoid sharp, knife-like pain; a “good-hurt” is okay! Next, do the same thing with light (one-finger) resistance in BOTH directions. Try three slow reps four to six times a day!
3) MUSCLE STRENGTH: Try pushing your head gently into your hand in the six directions listed above to provide a little resistance. Next, reach back with both hands or wrap a towel around your neck and pull forwards on the towel while you push the middle of your neck backwards into the towel doing the chin-tuck/glide maneuver (same as #1). Repeat three to five times slowly pushing, and more importantly, release the push slower! This is the MOST IMPORTANT of the strengthening exercises in most cases! Next, “squeeze” your shoulder blades together followed by spreading them as far apart as possible (repeat three to five times).
4) PERIODIC BREAKS: Set a timer to remind yourself to do a stretch, get up and move, to tuck your chin inwards (#1) and do some of #2 and #3 every 30-60 minutes.
5) LIFTING/CARRYING/WORK: Be SMART! Do not re-injure yourself. Change the way you handle yourself in your job, in the house, and while performing recreational activities.
6) HOUSEHOLD ACTIVITIES: Use a dolly to move boxes and keep commonly used items within easy reach (not too high or low).
Be smart, stay educated, work within the range your body tells you is “safe” and most importantly, STAY IN CONTROL!!!
Trigger points in the Levator scapula
The Levator scapula is a muscle in your neck that originates on the transverse processes of C1-C4 and inserts on the superior part of the medial border of the scapula. The primary actions of this muscle are to elevate the scapula and rotate the glenoid fossa downward. It also rotates the neck to the same side and assists in extension. When this muscle is tight it restricts neck rotation resulting in the classic “stiff neck”. With a forward head position the Levator is often stretched and over worked. To help combat this you must get the head back by releasing the anterior chest and neck muscles. Trigger points in this muscle refer pain into the angle of the neck and down the shoulder blade.
How can a low speed crash cause injury?
There is certainly a lot of interest in concussion these days between big screen movies, football, and other sports-related injuries. Concussion, traumatic brain injury (TBI), and mild traumatic brain injury (mTBI) are often used interchangeably. Though mTBI is NOT the first thing we think about in a low-speed motor vehicle collision (MVC), it does happen. So how often do MVC-related TBIs occur, how does one know they have it, and is it usually permanent or long lasting?
Here are some interesting statistics: 1) The incidence rate of fatal and hospitalized TBI in 1994 was estimated to be 91/100,000 (~1%); 2) Each year in the United States, for every person who dies from a brain injury, five are admitted to hospitals and an additional 26 seek treatment for TBI; 3) About 80% of TBIs are considered mild (mTBI); 4) Many mTBIs result from MVCs, but little is known or reported about the crash characteristics. 5) The majority (about 80%) of mTBI improve within three months, while 20% have symptoms for more than six months that can include memory issues, depression, and cognitive difficulty (formulating thought and staying on task). Long-term, unresolved TBI is often referred to as “post-concussive syndrome.”
In one study, researchers followed car crash victims who were admitted into the hospital and found 37.7% were diagnosed with TBI, of which the majority (79%) were defined as minor by a tool called Maximum Abbreviated Injury Scale (MAIS) with a score of one or two (out of a possible six) for head injuries. In contrast to more severe TBIs, mild TBIs occur more often in women, younger drivers, and those who were wearing seatbelts at the time of the crash. Mild TBI is also more prevalent in frontal vs. lateral (“T-bone”) crashes.
As stated previously, we don’t think about our brains being injured in a car crash as much as we do other areas of our body that may be injured—like the neck. In fact, MOST patients only talk about their pain, and their doctor of chiropractic has to specifically ask them about their brain-related symptoms.
How do you know if you have mTBI? An instrument called the Traumatic Brain Injury Questionnaire can be helpful as a screen and can be repeated to monitor improvement. Why does mTBI persist in the “unlucky” 20%? Advanced imaging has come a long way in helping show nerve damage associated with TBI such as DTI (diffuse tensor imaging), but it’s not quite yet readily available. Functional MRI (fMRI) and a type of PET scanning (FDG-PET) help as well, but brain profusion SPECT, which measures the blood flow within the brain and activity patterns at this time, seems the most sensitive.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honored to render our services.
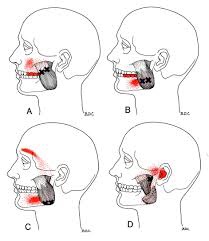
Trigger points in the masseter muscle

The masseter is the main muscle that moves your jaw. It originates on the zygomatic arch and maxilla, and inserts on the coronoid process and Ramus of the mandible. It’s actions are to elevate the mandible and close the jaw. The deep fibres of this muscle also retrude the mandible. This muscle commonly harbours trigger points as a result of teeth grinding. Trigger points in this muscle are often also associated with tmj dysfunction. Trigger points in the upper part of this muscle will refer pain to the upper molars and maxilla often felt as sinusitis. Trigger points in the lower portion of this muscle refer to the lower molars and temple. All trigger points can cause tooth sensitivity