The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
Sports
Pes Anserine Bursitis; What Is It?
The term “pes anserine” is Latin for goose’s foot, and describes the appearance of three tendons that converge and insert on the inner portion of your knee. The pes anserine bursa is a fluid-filled, friction-reducing cushion, sandwiched between these tendons and your leg bone.
Injuries or irritation can cause the lining of the bursa to produce too much fluid, resulting in painful swelling. Patients with knee osteoarthritis are likely to have chronic irritation of the pes anserine bursa. The condition is more common in overweight patients, diabetics, and females. Runners and athletes in sports that require rapid side-to-side movements (i.e. football, soccer, tennis, etc.) are more likely suffer from the condition. Swimmers who do the breast stroke commonly suffer from pes anserine bursitis.
 Symptoms include pain on the inner side of your knee, just below the joint. Your pain is probably worse when you stand up or walk stairs. Discomfort increases during activities that require side-to-side movements (i.e. tennis, dancing). Be sure to tell your doctor if you notice clicking, popping, or locking of your knee, excessive thirst, excessive urination, fever, or pain & swelling in your calf.
Symptoms include pain on the inner side of your knee, just below the joint. Your pain is probably worse when you stand up or walk stairs. Discomfort increases during activities that require side-to-side movements (i.e. tennis, dancing). Be sure to tell your doctor if you notice clicking, popping, or locking of your knee, excessive thirst, excessive urination, fever, or pain & swelling in your calf.
In addition to the treatment provided by our office, you may find relief by applying home ice or ice massage for 8-10 minutes. Having flat feet places additional stress on the inside of your knee, so patients with fallen arches will benefit from arch supports or orthotics. Overweight patients will benefit from a diet and exercise program.
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.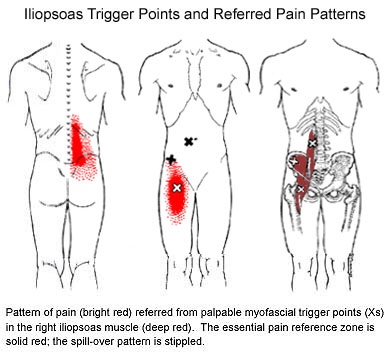
What is a “Mild” traumatic Brain Injury?
A concussion is a blow or jolt to the head that disrupts normal brain function. Concussions, also known as Mild Traumatic Brain Injuries, most often result from falls, sports injuries, and auto accidents.
 Concussion symptoms may begin immediately after an injury, but sometimes take hours or days to appear. The most common symptoms of a concussion include; headaches, light-headedness, dizziness, visual disturbances, ringing in the ears, confusion, fatigue, difficulty sleeping, irritability, and difficulty remembering or learning new things. Patients sometimes struggle to understand conversations or make simple calculations like determining a restaurant tip. Patients often feel as if they are “in a fog”. Symptoms can range from subtle to debilitating.
Concussion symptoms may begin immediately after an injury, but sometimes take hours or days to appear. The most common symptoms of a concussion include; headaches, light-headedness, dizziness, visual disturbances, ringing in the ears, confusion, fatigue, difficulty sleeping, irritability, and difficulty remembering or learning new things. Patients sometimes struggle to understand conversations or make simple calculations like determining a restaurant tip. Patients often feel as if they are “in a fog”. Symptoms can range from subtle to debilitating.
Patients and their attendants should be particularly alert for signs or symptoms that could indicate a more threatening injury like; worsening headache, growing irritability, repeated vomiting, difficulty speaking or swallowing, shortness of breath, unequal pupils, fever, visual disturbances, seizures, clear discharge from the nose or ears, loss of consciousness, or increasing light-headedness, numbness, or confusion. These symptoms warrant immediate emergency medical attention.
Recovery times are quite variable and are dependent upon a number of factors. It is critical that you allow your brain to recover completely before returning to physical activity. A concussion can be likened to dropping a computer – you will need to allow time to reboot before trying to use it. Suffering a second concussion before the first has completely resolved can lead to significantly worse symptoms and long-term impairments.
Athletes who have suffered a concussion must not return to activity before being evaluated by a healthcare professional that is very familiar with concussion management.
My abductors are weak, what does that mean?
One very important job of your hip muscles is to maintain the alignment of your leg when you move. One of the primary hip muscles, the gluteus medius, plays an especially important stabilizing role when you walk, run, or squat. The gluteus medius attaches your thigh bone to the crest of your hip. When you lift your left leg, your right gluteus medius must contract in order to keep your body from tipping toward the left. And when you are standing on a bent leg, your gluteus medius prevents that knee from diving into a “knock knee” or “valgus” position. 
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
You should avoid activities that cause prolonged stretching of the hip abductors, like “hanging on one hip” while standing, sitting crossed legged, and sleeping in a side-lying position with your top knee flexed and touching the bed. Patients with fallen arches may benefit from arch supports or orthotics. Obesity causes more stress to the hip muscles, so overweight patients may benefit from a diet and exercise program. The most important treatment for hip abductor weakness is strength training. Hip strengthening is directly linked to symptom improvement. Moreover, people with stronger hip muscles are less likely to become injured in the first place. The exercises listed below are critical for your recovery.
Meet the Hip Cycle. You can thank me later.
1. Side lying with back and shoulders against a wall so you can’t roll back.
2. Bend your bottom leg and put the sole of your foot against the wall to be more stable.
3. Start position is with your foot directly in line with your hip. Do not let it get any lower than that. The highest point of your foot needs to be the bump on the outside of your ankle.
Do 5-10 reps of each of the following without rest between exercises twice a day. The goal is 20 reps each.
a. 6″ leg raises in abduction
b. Knee up to chest (90* knee and hip)
c. 12″ leg raises into abduction
d. Bicycling (knee up to chest, extend knee and sweep back to start with leg straight)
e. Clockwise circles
f. Counterclockwise circles
Good luck.
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 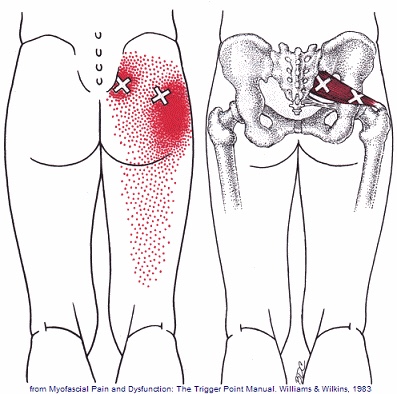
Scapular Dyskinesis (Yes, its a thing).
Your shoulder is formed by three bones; the scapula (shoulder blade), the clavicle (collar bone), and the humerus (long arm bone.) These bones come together to form a shallow ball & socket that relies upon the surrounding muscles for support. All of your shoulder muscles must work in a coordinated fashion to have a healthy and stable joint. Disruption of the normal rhythm of your shoulder blade creates abnormal strain on your shoulder and rotator cuff called “Scapular dyskinesis”. This dysfunction crowds the area of your shoulder where your rotator cuff tendons live and may create a painful pinching of your tendons or bursa each time you raise your arm. Many shoulder problems, including sprains/strains, tendinitis, bursitis, or rotator cuff irritation, result from this often overlooked culprit.

Scapular dyskinesis most commonly originates from weakness or imbalance of the muscles that control your shoulder blade. Sometimes the problem is caused by other shoulder conditions like prior fractures, arthritis, or instability. Irritation of the nerves that control the shoulder muscles is the culprit in about 5% of cases.
Although scapular dyskinesis can cause a variety of shoulder problems, it may initially go unnoticed. Up to 75% of healthy college athletes show some form of abnormal shoulder blade movement. If the condition is left untreated, you may begin to notice pain near the top of your shoulder. Sometimes the discomfort can radiate toward your neck or into your arm. Patients will often complain of a tender spot on the front of their shoulder. Long-standing altered mechanics can lead to bigger problems, including rotator cuff injury, shoulder instability, and arthritis.
The good news is that we have recognized the underlying cause of your shoulder problems and have treatments to correct it. You will need to perform your exercises consistently. You should also be conscious of your posture and try to avoid sitting or standing in “slouched” positions, as this is known to aggravate your problem.
Trigger points in the gluteus minimus
The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
The High Ankle Sprain (Don’t Let This Happen To You. These SUCK.)
Your lower leg bones (tibia and fibula) are held together at the ankle by a group of soft tissues and ligaments called the “syndesmosis”. This connection prevents excessive spreading of these bones during normal activity, but injuries can cause these ligaments to be stretched or torn. This problem is called a “syndesmotic ankle sprain” or “high ankle sprain”. High ankle sprains often occur during contact sports (like football, hockey, and soccer) when your foot is planted while the rest of your body shifts forward and turns inward. High ankle sprains are much less common than other types of ankle sprains.

The pain of a high ankle sprain starts just above your ankle and runs up your shin. Interestingly, the “length” of pain correlates very closely to your severity of injury. Standing and walking is usually uncomfortable and sometimes unbearable. Bringing your toes toward your shin or rotating your foot outward will likely increase your pain. Significant bruising or swelling is possible. Be sure to tell your doctor if you notice numbness, tingling, or coldness in your foot.
Ankles that have suffered a complete separation usually require surgery, since they will have lost the ability to push off, propel, and cut. Most other stable sprains will respond to conservative care, like the type provided in this office. It is important to recognize that high ankle sprains heal more slowly than other types of ankle sprains. The average recovery time for a syndesmotic sprain is between two and seven weeks but some injuries may require up to four months away from your sport. You may need to wear a boot or avoid weight bearing for a period of time. Ice may help to limit swelling initially, and the home exercises described below are an important part of your recovery.
