Myofascial pain syndrome (trigger points) and fibromyalgia are often confused to be the same condition and while there is a lot of interrelatedness between the two they are not quite identical. The clinical definition of a trigger point is “a hyper irritable spot associated within a taut band of skeletal muscle that is painful on compression or muscle contraction, and usually responds with a referred pain pattern distant from the spot”. Trigger points form from an overload trauma to the muscle tissue. This is contrasted with fibromyalgia which is defined as “a medical condition characterized by chronic widespread pain and a heightened pain response to pressure. Other symptoms include tiredness to a degree that normal activities are affected, sleep problems and troubles with memory. Some people also report restless leg syndrome, bowel and bladder problems, numbness and tingling and sensitivity to noise, lights and temperature. It is also associated with depression, anxiety, and post traumatic stress disorder”. Fibromyalgia will also present with localized tender points which are often mistaken for trigger points. Where these two conditions become somewhat interrelated is via the nervous system. Fibromyalgia patients suffer from a super-sensitization of the nervous system causing hyperirritability and pain. Myofascial trigger points can be caused by,or be the cause of, super sensitization. An active trigger point will irritate the sensory nerves around it eventually leading to super-sensitization. Trigger points have also been showed to form of become active due to super-sensitization. Both of these conditions can perpetuate the other, leading to layers of pain and symptoms. This being the case, trigger point therapy can have a very positive effect on decreasing the severity of pain and symptoms in patients suffering from fibromyalgia.

Seniors
Trigger points in the adductor longus and brevis.
These muscles are located in the groin. The longus originates on the pubic body just below the pubic crest and inserts on the middle third of the linea aspera.The brevis muscle originates on the inferior ramus and body of the pubis and has its attachment to the lesser trochanter and linea aspera of the femur. Trigger points in these muscles are the most common muscular cause of groin pain. Distal trigger points refer pain to the upper medial knee and down the tibia. Proximal trigger points refer into the anterior hip area.
Bryan Cobb RMT.
Since 2005, Bryan has been dedicated to helping all people with chronic and acute pain caused by soft-tissue damage.
His training and experience make him uniquely qualified to treat a wide variety of pain and dysfunction and to give instruction on prevention and self-care.
Bryan is the only Massage Therapist in Manitoba — and one of the few in Canada — to be certified by the Certification Board for Myofascial Trigger Point Therapists (CBMTPT).
Bryan holds a degree as an Advanced Remedial Massage Therapist (ARMT) from the Massage Therapy College of Manitoba. Course work at MTCM includes
• over 2,000 hours of practice, as well as
• intensive course work,
• a supervised clinical practicum, and
• community outreach placements.MTCM has a credit transfer affiliation with the University of Winnipeg, ensuring that its courses are held to the highest level. When Bryan studied at MTCM, the college was the only massage therapy college in western Canada accredited by the Commission on Massage Therapy Accreditation. Today, the college is a member of the Canadian Council of Massage Therapy Schools.
Bryan is a member in good standing of the Natural Health Practitioners of Canada.
Bryan also has a background in Anatomy, Exercise Physiology, and Sport Sciences from the University of Manitoba, and he has worked as a personal trainer and fitness leader.
He is an avid natural bodybuilder and fitness enthusiast, and has a blue belt in Brazilian jiu-jitsu.
Trigger points in the Quadratus Lumborum muscle.
The quadratus lumborum muscle is a commonly overlooked source of low back pain and is often responsible for “pseudo disc syndrome”. This muscle originates on the inferior border of the 12th rib and lumbar transverse processes. It inserts on the iliac crest and iliolumbar ligament. The q.l.’s main actions are extension and lateral flexion of the spine. It also acts as a stabilizer of the lumbar spine. Trigger points in this muscle refer pain into the sacroiliac joint and the lower buttock. Pain can also spread anteriorly along the crest of the ilium into the lower abdomen and groin and to the greater trochanter. 
Want a fancy new hip? Start with this!
A “joint” is an area where two or more bones come together. These bones have a slick rubbery protective covering, called “cartilage,” on the areas where they meet. This cartilage serves as a friction reducer and shock absorber, thereby prolonging the health of our joints.
Osteoarthritis, or simply arthritis, occurs when your joint cartilage degenerates as a result of repetitive stress.

Over time, this cartilage can thin and crack, eventually wearing away, leading to a painful “bone on bone” situation. Thinning of your joint cartilage is often accompanied by the development of “bone spurs” and/or joint deformity further disrupting your joint function.
Hip arthritis is common, affecting up to one-third of the population. The likelihood of you developing osteoarthritis increases as you age, and appears to be at least partially inherited from your parents. It is more common if you have been overweight and if you were subjected to repetitive injury, including occupations & sports requiring prolonged standing or heavy physical exertion.
An early symptom of Hip OA is prolonged stiffness upon arising in the morning and following periods of inactivity. You might complain of the inability to put your socks on, shave your legs or climb stairs. Groin, thigh and buttock pain are common. In some cases the pain can radiate into your lower leg. Cracking and popping of your hip when moving is possible.
It is sometimes difficult for doctors to differentiate between hip osteoarthritis and lower back problems that can also cause hip pain. Your doctor will likely X-ray your hip to determine the extent of your arthritis (graded 1-4 based on severity).
Arthritis cannot be cured, but your symptoms can often be relieved. Treatment of hip arthritis may include exercises, especially water-based programs like “water-aerobics.” Your doctor may use physical therapy modalities and will likely stretch and manipulate your hip, as this has been shown to be effective at relieving symptoms.
Your doctor may recommend that you avoid aggravating activities, especially those requiring you to rotate your hip internally (i.e., pigeon toed” movements), and to maintain a healthy weight. You will be taught home stretching and strengthening exercises to help you recover. Taking 1500 mg of Glucosamine and chondroitin has been shown to help some arthritis sufferers.
In more severe cases, you may need to use a cane (in the opposite hand) to take weight off the arthritic hip. If conservative treatment fails to relieve your pain, your doctor might recommend consultation with an orthopedic hip specialist to consider joint replacement.
Trigger points in the temporalis muscle
The temporalis muscle is located in the temple area of the skull. It originates on the temporal lines on the parietal bone of the skull, and inserts on the coronoid process of the mandible. It’s main action is to close the jaw. The posterior and middle fibres bilaterally retrude the mandible. Acting individually, this muscle will deviate the mandible to the same side. Trigger points in this muscle refer into the teeth causing hypersensitivity, and into and above the eye and temple, causing headaches.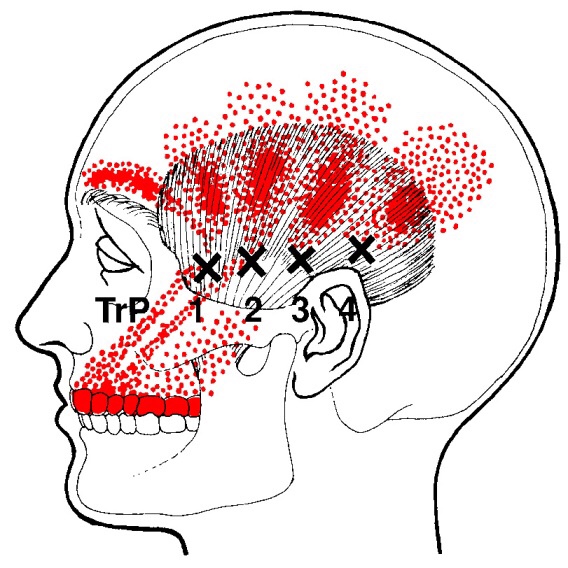
Trigger points in the serratus anterior
The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
There is nothing great about greater trochanteric pain syndrome. Nothing at all.
Your hip typically has about six small fluid-filled sacs called “bursa” that act as cushions between tendons and bone. One of the most common causes of hip pain is a condition called, “hip bursitis” which means that one or more of your bursas have become painfully inflamed. The broader (more accurate) diagnosis of “Greater trochanteric pain syndrome” (GTPS) describes an uncomfortable collection of problems affecting the outermost portion of your hip. GTPS can include swelling of one or more of the fibrous tendons that attach your muscles onto your hip – a condition called, “tendinitis.” In addition to bursitis & tendonitis, GTPS may originate from tightness in the muscle that travels over your hip en route to your knee- resulting in compression and irritation to your hip.

Greater trochanteric pain syndrome is most common in middle age to elderly adults and is 2-4 times more common in females. Sometimes the problem affects both hips at the same time. Approximately 1/3 of patients with GTPS have lower back pain. Patients who have arthritis in their hips and knees are more likely to suffer from ongoing complaints.
Your symptoms probably include a persistent pain on the outside of your hip, buttock, and upper thigh. Your discomfort may be aggravated by sitting with your leg crossed, arising from a seated position, prolonged standing, climbing stairs, and high-impact activities, like running. Sometimes patients find it difficult to sleep, since lying on the painful hip usually increases symptoms.
For adults, x-rays may or may not be needed to confirm the diagnosis, but children and adolescents usually require films to rule out more serious childhood diseases. Be sure to tell your doctor if you notice that you have a fever, leg numbness, pain radiating significantly beyond your knee, or pain in the front of your groin crease (the area where you leg meets your pelvis.)
Conservative treatment, like the type provided in this office, is successful in about 90% of cases. If you have acute pain, you may need to temporarily limit or discontinue activities that increase your discomfort. Using ice or ice massage at home may help. Some patients find temporarily relief by applying sports creams. Very commonly, patients with pain on the outside of their hip suffer from weakness in one of their buttock muscles, called the “gluteus medius.” When this muscle lacks strength, it is unable to protect your hip during normal activities, like walking. Research has shown that strengthening your hip has a dramatic effect on your progress.
Athletes should avoid running on a banked surface, like the crown of a road or indoor track. Be sure to reverse directions each mile if you run on a circular track. Avoid running on wet or icy surfaces, as this can cause increased tension in your hip. Runners with a “lazy” narrow-based running gait will benefit by increasing their step width to minimize stress on their hip. Cyclists need to make sure that their seat is not positioned too high. Overweight patients should consider weight reduction programs.
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.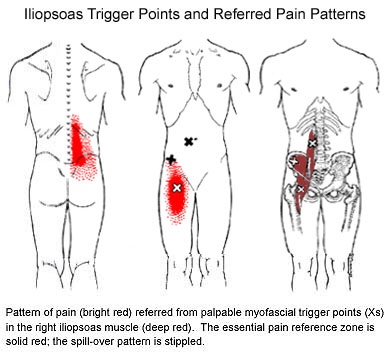
What is Fibromyalgia?
Fibromyalgia, although often misdiagnosed and misunderstood, is the second most common musculoskeletal disorder behind osteoarthritis. The condition affects nearly 12 million Americans and is ten times more common in women.
The diagnosis of fibromyalgia is made when a certain set of symptoms has been present for at least three months. The most common symptoms include wide-spread muscle and joint pain, achiness or soreness- especially in the neck, shoulders, back, and hips. Your muscles may constantly feel overworked and tired. Fibromyalgia patients often exhibit a set of predictable “tender points” spread throughout the body. Some patients have trouble sleeping and feel as though they are in a “brain fog” most of the day. This can lead to fatigue or mood changes, like anxiety and depression.

Stress is a known contributor to fibromyalgia, and patients should seek ways to de-stress, including yoga or meditation. Fibromyalgia patients should minimize their caffeine intake, as this is a known stimulant for nervousness, anxiety, and insomnia. Breathing exercises are sometimes helpful.
Although your sleep may be restless, you should try to establish a bedtime routine that gives your body the best chance for recovery. Try to avoid late night electronics, like the television or computer. Keep your bedroom dark, quiet, cool, and distraction-free. Be sure to take time for yourself each day for relaxation or to do something you enjoy. Combat “brain fog” by carrying a notebook or a phone to make notes for important things. Some patients report decreased muscle tightness by applying moist heat or a taking warm bath. The American Pain Society recommends conservative treatment, including chiropractic, along with moderate aerobic exercise.
