This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.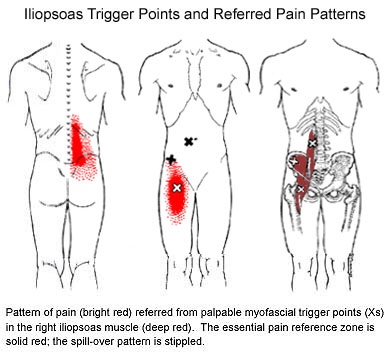
Physio
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 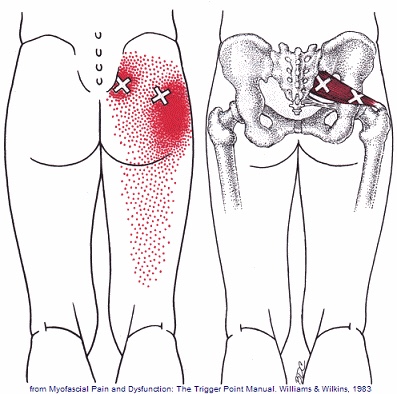
Scapular Dyskinesis (Yes, its a thing).
Your shoulder is formed by three bones; the scapula (shoulder blade), the clavicle (collar bone), and the humerus (long arm bone.) These bones come together to form a shallow ball & socket that relies upon the surrounding muscles for support. All of your shoulder muscles must work in a coordinated fashion to have a healthy and stable joint. Disruption of the normal rhythm of your shoulder blade creates abnormal strain on your shoulder and rotator cuff called “Scapular dyskinesis”. This dysfunction crowds the area of your shoulder where your rotator cuff tendons live and may create a painful pinching of your tendons or bursa each time you raise your arm. Many shoulder problems, including sprains/strains, tendinitis, bursitis, or rotator cuff irritation, result from this often overlooked culprit.

Scapular dyskinesis most commonly originates from weakness or imbalance of the muscles that control your shoulder blade. Sometimes the problem is caused by other shoulder conditions like prior fractures, arthritis, or instability. Irritation of the nerves that control the shoulder muscles is the culprit in about 5% of cases.
Although scapular dyskinesis can cause a variety of shoulder problems, it may initially go unnoticed. Up to 75% of healthy college athletes show some form of abnormal shoulder blade movement. If the condition is left untreated, you may begin to notice pain near the top of your shoulder. Sometimes the discomfort can radiate toward your neck or into your arm. Patients will often complain of a tender spot on the front of their shoulder. Long-standing altered mechanics can lead to bigger problems, including rotator cuff injury, shoulder instability, and arthritis.
The good news is that we have recognized the underlying cause of your shoulder problems and have treatments to correct it. You will need to perform your exercises consistently. You should also be conscious of your posture and try to avoid sitting or standing in “slouched” positions, as this is known to aggravate your problem.
Trigger points in the gluteus minimus
The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
Trigger points in the gluteus Maximus
The gluteus Maximus is the buttock muscle. It originates on the gluteal surface of the ilium, lumbar fascia, sacrum and sacrotuberous ligament. It inserts on the gluteal tuberosity of the femur and the iliotibial tract. Extension and lateral rotation of the hip are it’s main actions. This muscle is heavily involved in activities like ice skating and is a common area to develops trigger points. When trigger points do develop they can refer pain in a crescent pattern from the gluteal fold to the sacrum. Trigger points can also refer pain deep into the buttock itself making it feel like other deeper muscles are involved. These symptoms can sometimes be mistaken for s.i. Joint problems. 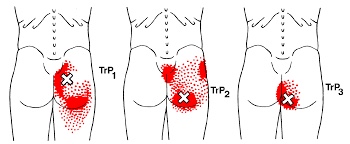
Trigger points in the supraspinatus
The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.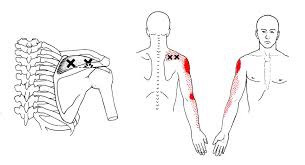
Can Chiro help me?

Chiropractic is the most widely accepted and most frequently used type of “alternative” healthcare in the United States. This is largely due to the fact that it works, and because of that, there has been a steady increase in acceptance by the public, third-party payers, and the Federal government. Since the mid-1990s, a number of outside (non-chiropractic) observers have suggested that chiropractic has now entered mainstream healthcare.
One can position chiropractic as being BOTH alternative and mainstream. It is “alternative” since it approaches healthcare from an entirely different direction compared to the primary care medical profession. Chiropractic is non-surgical and promotes diet and nutritional approaches vs. drugs and surgery. Chiropractic is also arguably “mainstream” as it has evolved into a strongly utilized form of primary care through popular acceptance and utilization by the public.
So, what role does chiropractic play in today’s health delivery system? This question is still being debated, but there appears to be three camps: 1) Specialist—limited to musculoskeletal (MSK) complaints on an interdisciplinary primary healthcare team; 2) Primary healthcare “gatekeepers” that focus on ambulatory MSK complaints; 3) Generalist primary healthcare provider of “alternative or complementary” medicine that manage and/or co-manage both MSK AND non-MSK conditions.
Looking at this from the patient or “consumer” perspective, chiropractic already plays an important role in the healthcare delivery for many patients. In 1993, a report claimed 7% of American adults had received chiropractic care during the prior year. According to a 2015 Gallup poll (that included 5,442 adults, aged 18+, surveyed between 2/16/15 and 5/6/15) entitled, Majority in U.S. Say Chiropractic Works for Neck, Back Pain, “Chiropractic care has a positive reputation among many US adults for effective treatment of neck and back pain, with about six in 10 adults either strongly agreeing (23%) or agreeing somewhat (38%) that chiropractors are effective at treating these types of pain.”
The “highlights” from this Gallup poll include: 1) Two-thirds say chiropractic is effective for neck and back pain. 2) Many adults say chiropractors think of the patient’s best interest. 3) More than 33 million adults in the United States (US) saw a chiropractor in the twelve months before the survey was conducted. That means roughly 14% of U.S. adults saw a chiropractor in the 12 months prior to the survey (vs. 7% in 1993). An additional 12% who responded to the Gallup pollsters saw a chiropractor in the last five years but not in the last 12 months. Overall, 51% of those polled had previously seen a chiropractor.
Whether or not you have personally utilized chiropractic, the educational process, licensing requirements, public interest, third-party payer systems, and interprofessional cooperation ALL support firm ground for which you can comfortably and confidently seek chiropractic care for your complaints.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care, we would be honored to render our services.
Trigger points in the infraspinatus
The infraspinatus muscle is one of the muscles that makes up the rotator cuff. It originates on the infraspinous fossa of the scapula, and inserts on the middle facet of the greater tubercle of the humerus. It functions to externally rotate the humerus and to stabilize the head of the humerus in the glenoid cavity during upward movement of the arm. Trigger points in this muscle refer pain deep into the anterior shoulder joint and down the anterior arm. Trigger points near the lower medial border refer pain into the rhomboids. This muscle is often injured during throwing motions.
What is Scoliosis?

Your spine is made up of 24 bones that stack on top of each other- normally in a straight line. “Scoliosis” means that your spine is curving from side to side, rather than being straight. Scoliosis affects between 1-3% of the population. Scoliosis may begin at any time between birth and adulthood but is most common during times that your skeleton is growing rapidly. Most cases of scoliosis begin between the ages of 13 and 18. Researchers are not completely certain why some people develop scoliosis, but they have found that the problem tends to run in families.
The curve of your scoliosis may be measured with an x-ray. Although some curves get worse, most do not. In fact, only ¼ of all adolescent idiopathic scoliosis curves will progress. Small curves in mature patients have a low risk of progression (2%), while large curves in younger patients progress more frequently. (70%) Curve progression is more common in girls, especially those with larger curves (greater than 20 degrees). Your doctor may need to monitor your scoliosis for progression by performing x-rays every 6-18 months.
Scoliosis may cause your shoulders, hips, or waist to be unlevel. Most curves are classified as “right thoracic”, which means that the peak of your curve protrudes toward the right. This is often accompanied by a forward rotation of your right shoulder and “winging” of your right shoulder blade. Many patients have a secondary curve in their lower spine that helps to balance their body. The majority of patients with mild to moderate scoliosis have no symptoms, but approximately ¼ report back pain. Unfortunately, scoliosis increases your risk of developing back pain later in life.
The primary goal of treatment is to stop curve progression. While many cases can be slowed or even reversed through appropriate management, it is important to recognize that others may progress in spite of the best care. Conservative care, including spinal manipulation (like the type provided in our office) has been shown to help some patients with scoliosis. Exercise is another effective treatment for scoliosis. It is important that you clearly understand your home exercise program and that you perform it consistently.
Patients with larger curves (30-40 degrees), or those who are at high risk for progression may benefit from wearing a brace. Braces have been shown to decrease the need for surgery in about three out of four patients. Fortunately, less than 0.3% of all scoliosis cases will ever require surgery.
You should avoid carrying heavy back packs and consider switching to a wheeled version, if necessary. Sports and exercise will not worsen most cases of scoliosis, and you should continue to participate in the things you enjoy unless directed otherwise by your doctor. The diagnosis of scoliosis is always discouraging, but you must focus on what it is really most important. Be confident in who you are! Don’t let something like a curved spine (or any other medical condition) define you as a person.
