In a 2010 study, researchers examined MRIs taken from 1,200 patients (600 whiplash and 600 non-whiplash neck pain patients) and noted that those who had sustained whiplash were more likely to have a brain injury than non-whiplash neck pain patients.
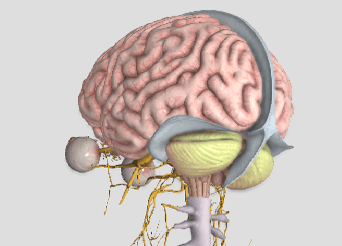
The specific type of brain injury found is a form of herniation called Chiari malformation, where the bottom part of the brain (the cerebellum) drops through the opening in the base of the skull called the foramen magnum. Their findings showed an alarming 23% of the whiplash cases studied had this anatomical abnormality.
Dr. Michael Freeman, Dr. Ezriel Kormel, and colleagues collaborated in this effort and evaluated the patients using MRI in both recumbent (laying down) AND upright positions. Interestingly, they found 5.7% and 5.3% of those in the non-whiplash neck pain group and 9.8% and 23.3% in the whiplash group had the Chiari malformation using the recumbent vs. upright MRI positions, respectfully.
Dr. Kormel stated, “This condition can be quite painful and endanger the patient’s health, with symptoms that may include headaches, neck pain, upper extremity numbness and tingling, and weakness. In a few cases, there can also be lower extremity weakness and brain dysfunction.” In a radio interview, he added the advice that ANYONE suffering from whiplash should see a healthcare provider immediately.
This study is important for a number of reasons. First, it revealed that there is often a more serious injury when whiplash occurs than what is initially found. Second, psychological findings like depression, anxiety, and difficulty coping with the decreased ability or inability to be productive at home or work may suggest the presence of an anatomical injury which simply has not yet been found. Third, MRI is frequently ONLY performed in a laying down position. This study didn’t find much difference between laying vs. weight-bearing MRI positions in the non-whiplash neck pain patients but not so in the whiplash neck pain group! In this group, the ability for MRI to detect Chiari malformation/brain injury more than doubled using weight-bearing MRI.
Expanding the last point, since one out of five whiplash patients had a brain injury that is more likely to be detected using a non-traditional upright MRI position, a “new” standard” for the use of MRI in the evaluation of the whiplash patient should be considered. This is especially important in those cases that are non-responsive to quality care or if their doctor had only ordered a recumbent MRI previously.