The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
Physio
How long does Whiplash last?

First, what is whiplash? It’s a lot of things, which is why the term WAD or Whiplash Associated Disorders has become the most common term for the main signs and symptoms associated with a whiplash injury. WAD is usually associated with a motor vehicle collision, but sports injuries, diving accidents, and falls are other common ways to sustain a WAD injury.
To answer the question of the month, in most cases, the recovery rate is high and favors those who resume their normal daily activities. The worse thing you can do when you sustain a WAD injury is to not do anything! Too much rest and inactivity leads to long-term disability. Of course, this must be balanced with the degree of injury, but even when the injury requires some “down time,” stay as active as possible during the healing phase.
Many people recover within a few days or weeks while a smaller percentage require months and about 10% may only partially recover. So what can be done to give you the best possible chance to fully recover as soon as possible?
During recovery, you can expect your condition to fluctuate in intensity so “listen” to your body, let it “guide” you during activity and exercise, and stay within “a reasonable boundary of pain” during your activity. Remember, your best chance for full recovery FAVORS continuing a normal lifestyle. Make reasonable modifications so you can work, socialize, and do your “normal” activities!
The KEY: Stay in control of your condition – DO NOT let it control you! Here are some tips:
1) POSTURE CONTROL: Keep the weight of the head back by gliding your chin back until you “hit” a firm end-point. Then release it slightly so it’s comfortable—this is your NEW head position!
2) FLEXIBILITY: Try this range of motion (ROM) exercise… Slowly flex your neck forwards and then backwards, then bend your neck to the left and then the right, and then rotate it to the left and to then to the right. THINK about each motion and avoid sharp, knife-like pain; a “good-hurt” is okay! Next, do the same thing with light (one-finger) resistance in BOTH directions. Try three slow reps four to six times a day!
3) MUSCLE STRENGTH: Try pushing your head gently into your hand in the six directions listed above to provide a little resistance. Next, reach back with both hands or wrap a towel around your neck and pull forwards on the towel while you push the middle of your neck backwards into the towel doing the chin-tuck/glide maneuver (same as #1). Repeat three to five times slowly pushing, and more importantly, release the push slower! This is the MOST IMPORTANT of the strengthening exercises in most cases! Next, “squeeze” your shoulder blades together followed by spreading them as far apart as possible (repeat three to five times).
4) PERIODIC BREAKS: Set a timer to remind yourself to do a stretch, get up and move, to tuck your chin inwards (#1) and do some of #2 and #3 every 30-60 minutes.
5) LIFTING/CARRYING/WORK: Be SMART! Do not re-injure yourself. Change the way you handle yourself in your job, in the house, and while performing recreational activities.
6) HOUSEHOLD ACTIVITIES: Use a dolly to move boxes and keep commonly used items within easy reach (not too high or low).
Be smart, stay educated, work within the range your body tells you is “safe” and most importantly, STAY IN CONTROL!!!
My back hurts, why look at my feet?

Improperly supported feet can affect the alignment of all of the structures above. To improve your overall comfort:
✓ Choose shoes with good arch support.
✓ Avoid going barefoot or wearing shoes that lack support (i.e. flip-flops). The following brands of sandals provide better than average arch support: Naot, Fit Flops, Orthoheels, Abeo, Vionic and Yellow box.
✓ Avoid high-heeled shoes or boots (keep heels to a maximum of 1½ inches, especially if you are going to be doing a lot of walking).
✓ “Cross-trainer” athletic shoes tend to provide the best all around support and shock absorption for daily activities.
✓ Patients with fallen arches should consider adding arch supports or orthotics.
✓ Repair or replace shoes with worn soles or heels.
Lifting Mechanics Made Simple

Here are some tips to help you lift safely:
✓ Avoid lifting or flexing before you’ve had the chance to warm up your muscles (especially when you first awaken or after sitting or stooping for a period of time).
✓ To lift, stand close directly facing object with your feet shoulder width apart.
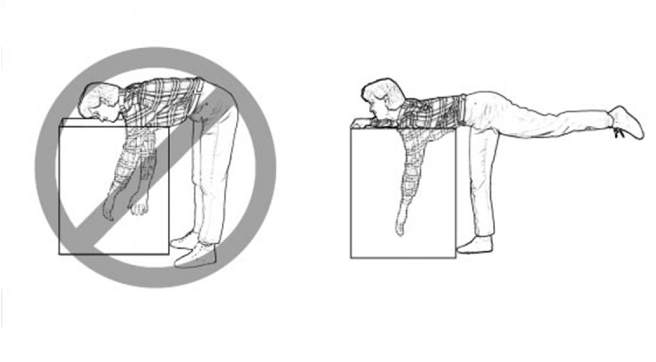
✓ Squat down by bending with your knees, not your back. Imagine a fluorescent light tube strapped to your head and hips when bending. Don’t “break” the tube with improper movements. Tuck your chin to help keep your spine aligned.
✓ Slowly lift by thrusting your hips forward while straightening your legs.
✓ Keep the object close to your body, within your powerzone” between your hips and chest. Do not twist your body, if you must turn while carrying an object, reposition your feet, not your torso.
An alternative lifting technique for smaller objects is the golfers lift. Swing one leg directly behind you. Keep your back straight while your body leans forward. Placing one hand on your thigh or a sturdy object may help.
Why do so many suffer with CTS?
According to the literature, carpal Tunnel Syndrome (CTS) is one of the most prevalent upper extremity complaints. In fact, it IS the most common “compression neuropathy” (of which there are many) and affects 3-6% of adults in the general population. Additionally, CTS can affect BOTH hands in up to 50% of patients with the condition!
The CAUSE of CTS is often unknown and typically comes on gradually, making it difficult to determine a definite cause or specific “date of onset” for CTS.
Symptoms such as numbness, tingling, loss of dexterity, loss of strength (like pinch or grip), and the need to shake the hand or flick the fingers to restore sensation are ALL VERY COMMON CTS SYMPTOMS. The REASON for these symptoms boils down to one thing: The median nerve in the wrist gets pinched! The cause/s can include:
1) Repetitive motion from either work or hobbies like assembly line work or playing a musical instrument can cause swelling within the carpal tunnel, placing extra pressure on the median nerve as it passes through.
2) Obesity can contribute to CTS due to extra fluids or fatty deposits that can build up within the carpal tunnel.
3) Pregnancy: Elevated levels of the hormones estrogen and progesterone can cause the body to retain fluids and increase pressure in the carpal tunnel.
4) Arthritis: Osteoarthritis can lead to CTS (such as when a spur forms inside the tunnel). Rheumatoid arthritis can lead to an autoimmune response and antibodies that end up attacking the cartilage of the joints in the wrist, which can lead to CTS.
5) Hormone-related conditions: In diabetes mellitus, the blood becomes thicker due to high sugar levels (like syrup) and can’t pass through the small blood vessels, resulting in “neuropathy,” which can make CTS more likely. In hypothyroid, low thyroid function results in “myxedema,” a specific type of swelling that makes CTS more likely to occur.
6) Trauma: A wrist fracture could cause the carpal tunnel to “collapse” or change in shape resulting in less space for the nerve to travel through.
7) Mass lesions: A “ganglionic cyst” is a good example. This is where joint fluid leaks out and forms a “bump” on the INSIDE the carpal tunnel, which reduces space and increases pressure in this anatomical structure.
8) Amyloidosis: This is a rare condition where a protein substance called “amyloid” builds up in any tissue or organ. If this occurs in the wrist, it can “pinch” the median nerve as it passes through.
9) Sarcoidosis: This is the growth of small collections of inflammatory cells called “granulomas,” which can accumulate in different parts of the body. If it occurs in the wrist, pinching can occur.
10) Multiple Myeloma: This is a type of cancer that affects the bone marrow, and inflammation in the wrist can occur creating the pressure increase on the median nerve that can lead to CTS.
11) Leukemia: This too is a type of cancer that involves the white blood cells, and CTS can result from its effects on the tissues in the wrist.
12) Anatomy: The size and shape of the carpal tunnel is hereditary, and some of us have a smaller tunnel than others. If CTS is present in multiple family members, this “genetic” factor may play a role.
There are other conditions that can “mimic” CTS, but doctors of chiropractic are trained to perform an accurate history and examination so treatment can be directed in the proper manner!
How can a low speed crash cause injury?
There is certainly a lot of interest in concussion these days between big screen movies, football, and other sports-related injuries. Concussion, traumatic brain injury (TBI), and mild traumatic brain injury (mTBI) are often used interchangeably. Though mTBI is NOT the first thing we think about in a low-speed motor vehicle collision (MVC), it does happen. So how often do MVC-related TBIs occur, how does one know they have it, and is it usually permanent or long lasting?
Here are some interesting statistics: 1) The incidence rate of fatal and hospitalized TBI in 1994 was estimated to be 91/100,000 (~1%); 2) Each year in the United States, for every person who dies from a brain injury, five are admitted to hospitals and an additional 26 seek treatment for TBI; 3) About 80% of TBIs are considered mild (mTBI); 4) Many mTBIs result from MVCs, but little is known or reported about the crash characteristics. 5) The majority (about 80%) of mTBI improve within three months, while 20% have symptoms for more than six months that can include memory issues, depression, and cognitive difficulty (formulating thought and staying on task). Long-term, unresolved TBI is often referred to as “post-concussive syndrome.”
In one study, researchers followed car crash victims who were admitted into the hospital and found 37.7% were diagnosed with TBI, of which the majority (79%) were defined as minor by a tool called Maximum Abbreviated Injury Scale (MAIS) with a score of one or two (out of a possible six) for head injuries. In contrast to more severe TBIs, mild TBIs occur more often in women, younger drivers, and those who were wearing seatbelts at the time of the crash. Mild TBI is also more prevalent in frontal vs. lateral (“T-bone”) crashes.
As stated previously, we don’t think about our brains being injured in a car crash as much as we do other areas of our body that may be injured—like the neck. In fact, MOST patients only talk about their pain, and their doctor of chiropractic has to specifically ask them about their brain-related symptoms.
How do you know if you have mTBI? An instrument called the Traumatic Brain Injury Questionnaire can be helpful as a screen and can be repeated to monitor improvement. Why does mTBI persist in the “unlucky” 20%? Advanced imaging has come a long way in helping show nerve damage associated with TBI such as DTI (diffuse tensor imaging), but it’s not quite yet readily available. Functional MRI (fMRI) and a type of PET scanning (FDG-PET) help as well, but brain profusion SPECT, which measures the blood flow within the brain and activity patterns at this time, seems the most sensitive.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honored to render our services.
Trigger points in the masseter muscle

The masseter is the main muscle that moves your jaw. It originates on the zygomatic arch and maxilla, and inserts on the coronoid process and Ramus of the mandible. It’s actions are to elevate the mandible and close the jaw. The deep fibres of this muscle also retrude the mandible. This muscle commonly harbours trigger points as a result of teeth grinding. Trigger points in this muscle are often also associated with tmj dysfunction. Trigger points in the upper part of this muscle will refer pain to the upper molars and maxilla often felt as sinusitis. Trigger points in the lower portion of this muscle refer to the lower molars and temple. All trigger points can cause tooth sensitivity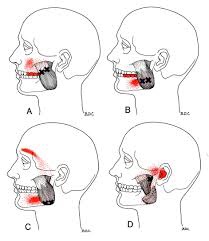
So I’ve got Whiplash; now what?
Whiplash, or “Whiplash Associated Disorders” or WAD, is the result of a sudden “crack the whip” of the head on the neck due to a slip and fall, sports injury, a violent act, or most commonly, a motor vehicle collision (MVC), particularly a rear-end collision. In describing “what can I expect” after a whiplash injury, one thing is for certain, there are many faces of whiplash, meaning the degree of injury can range from none to catastrophic depending on many factors, some of which are difficult or impossible to identify or calculate. Let’s take a closer look!
Even though the good news is that most people injured in a car crash get better, 10% do not and go on to have chronic pain, of which about half have significant difficulty working and/or doing desired everyday activities. There is a “great debate” as to the way experts describe “chronic whiplash syndrome” (CWS) as well as how these cases should be managed. Some feel there is something PHYSICALLY wrong in the CWS patient, especially if severe neck or head pain persists for more than one year. There is some proof of this as Dr. Nikolai Bogduk from the University of Newcastle in Australia and colleagues have used selective nerve blocks to anesthetize specific joints in the neck to determine exactly where the pain is generated. The patient then has the option to have that nerve cauterized or burned and pain relief can be significant in many cases. Dr. Bogduk and his group admit that these CWS patients have more psychological symptoms, but they feel this is the result of pain, not the CAUSE.
On the other hand, experts such as Dr. Henry Berry from the University of Toronto report the EXACT OPPOSITE. He argues that it’s not JUST the physical injury that has to be dealt with but also the person’s “state of mind.” Dr. Berry states that when stepping back and looking at all the complaints or symptoms from a distance, “…you see these symptoms can be caused by life stress, the illness ‘role’ as a way of adjusting to life, psychiatric disorders, or even [made up by the patient].” Berry contends that it’s important to tell the patient their pain will go away soon, advises NO MORE THAN two weeks of physical therapy, and sends people back to work ASAP.
Oregon Health Sciences University School of Medicine’s Dr. Michael D. Freeman, whose expertise lay in epidemiology and forensic science, disagrees with Dr. Berry stating that the scientific literature clearly supports the physical injury concept and states, “…the idea that it is a psychological disturbance is a myth that has been perpetuated with absolutely no scientific basis at all.” Dr. Freeman states that 45% of people with chronic neck pain were injured in a motor vehicle crash (which includes three million of the six million of those injured in car crashes every year in the United States).
Here’s the “take home” to consider: 1) CWS occurs in about 10% of rear-end collisions; 2) Some doctors feel the pain is physically generated from specific nerves inside the neck joints; 3) Others argue it’s a combination of psychological factors and care should focus on preventing sufferers from becoming chronic patients.
Many studies report that chiropractic offers fast, cost-effective benefits for whiplash-injured patients with faster return to work times and higher levels of patient satisfaction.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honored to render our services.
Up Close & Personal With Headaches.

Headaches are REALLY common! In fact, two out of three children will have a headache by the time they are fifteen years old, and more than 90% of adults will experience a headache at some point in their life. It appears safe to say that almost ALL of us will have firsthand knowledge of what a headache is like sooner or later!
Certain types of headaches run in families (due to genetics), and headaches can occur during different stages of life. Some have a consistent pattern, while others do not. To make this even more complicated, it’s not uncommon to have more than one type of headache at the same time!
Headaches can vary in frequency and intensity, as some people can have several headaches in one day that come and go, while others have multiple headaches per month or maybe only one or two a year. Headaches may be continuous and last for days or weeks and may or may not fluctuate in intensity.
For some, lying down in a dark, quiet room is a must. For others, life can continue on like normal. Headaches are a major reason for missed work or school days as well as for doctor visits. The “cost” of headaches is enormous—running into the billions of dollars per year in the United States (US) in both direct costs and productivity losses. Indirect costs such as the potential future costs in children with headaches who miss school and the associated interference with their academic progress are much more difficult to calculate.
There are MANY types of headaches, which are classified into types. With each type, there is a different cause or group of causes. For example, migraine headaches, which affect about 12% of the US population (both children and adults), are vascular in nature—where the blood vessels dilate or enlarge and irritate nerve-sensitive tissues inside the head. This usually results in throbbing, pulsating pain often on one side of the head and can include nausea and/or vomiting. Some migraine sufferers have an “aura” such as a flashing or bright light that occurs within 10-15 minutes prior to the onset while other migraine sufferers do not have an aura.
The tension-type headache is the most common type and as the name implies, is triggered by stress or some type of tension. The intensity ranges between mild and severe, usually on both sides of the head and often begin during adolescence and peak around age 30, affecting women slightly more than men. These can be episodic (come and go, ten to fifteen times a month, lasting 30 min. to several days) or chronic (more than fifteen times a month over a three-month period).
There are many other types of headaches that may be primary or secondary—when caused by an underlying illness or condition. The GOOD news is chiropractic care is often extremely helpful in managing headaches of all varieties and should be included in the healthcare team when management requires a multidisciplinary treatment approach.
Most of know someone who has been affected by headaches. If they are looking for help and information please feel free to contact us at 204-586-8424 or at info@aberdeenchiropractic.com.
Mind = Blown
Carpal tunnel syndrome (CTS) is a very common condition. According to a report by the Bureau of Labor Statistics (BLS), CTS ranks SECOND among the major disabling diseases and illnesses in ALL private industries. The BLS states that workers with CTS may eventually have to give up their livelihood. They cite one study in which almost half of all CTS patients changed their jobs within 30 months following their diagnosis. Due to the controversy surrounding the issue of CTS and worker’s compensation, workers do not always receive compensation benefits.
The KEY to long-term cost containment associated with CTS is EARLY DIAGNOSIS and PREVENTION! The challenge is getting the worker to identify early symptoms and NOT feel intimidated to report them, which could then lead to prompt care and possibly job modifications, resulting in the best chance of preventing a more complicated and far more costly problem.
Because of the many factors that contribute to and/or cause CTS, there is similarly no one way to prevent it from happening. Treating any/all underlying medical condition(s) is important. Using simple common sense can go a long way to help minimize some of the risk factors that predispose a person to work-related CTS and other cumulative trauma disorders (CTDs).
For example, watching and mimicking veteran workers can be a great guide as to how to maximize efficient work methods while minimizing unnecessary stresses and strains. Other preventative “tricks” include learning how to adjust the work area, handle tools, or perform tasks that minimize hand/wrist strain. Maintaining proper posture and exercise programs to strengthen the fingers, hands, wrists, forearms, shoulders, and neck may also help prevent CTS.
Many companies have taken action to help prevent repetitive stress injuries. In one study, 84% of the companies surveyed reported that they were modifying equipment, tasks, and processes as part of a prevention effort; nearly 85% analyzed their workstations and jobs; and 79% purchased more ergonomic equipment. Unfortunately, there is NO EVIDENCE that any of these methods can completely protect a worker against CTS. Often, the best approach is to relocate the worker to a less repetitive job, but this is not always an option.
Doctors of chiropractic can observe the worker through a video or during a factory tour/visit and often identify ergonomic problems that can result in a low-cost, easy modification. Simple modifications coupled with quality care, patient education, and cooperation from BOTH the worker and the employer can typically help yield the best outcome for the CTS patient.

