Carpal tunnel syndrome (CTS) is the most common of the many “entrapment neuropathies”— nerve pinches in the arms or legs—likely because we use our hands and fingers repetitively for long time frames at work and during many of our hobbies. In addition, the wrist is a very complicated joint because it’s not a simple ball-and-socket or hinge, like the hip, elbow, or knee.
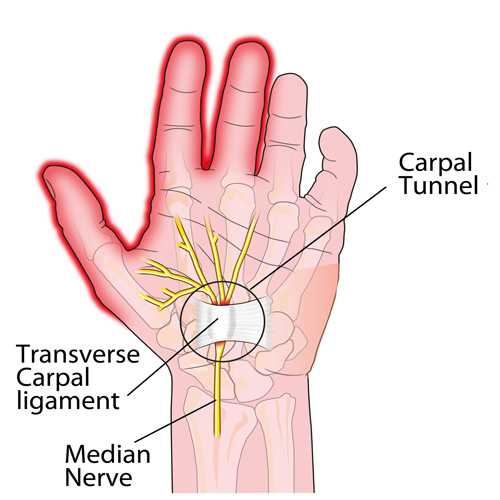
The wrist is made up of eight small “carpal” bones that are all shaped very differently and fit together a bit like a puzzle. These eight bones are lined up in two rows of four bones that form the “roof“ of the tunnel.
The shape of the tunnel changes with different activities, and the contents within the tunnel have to accommodate for this. Nine of the tendons that allow the hand to move the fingers also travel through the tunnel. Look at the palm-side of your wrist as you wiggle your fingers. See all the activity going on there? The median nerve travels through the tunnel as well, just under the “floor”, which is a very strong ligament that stretches from the pinky to the thumb-side of the tunnel.
Virtually ANY condition that increases the pressure inside the already tightly packed tunnel can create CTS symptoms like numbness, tingling, burning, etc. Over time, grip strength may weaken, causing one to accidentally drop objects.
To add to the causation list of CTS, conditions like obesity, pregnancy, diabetes, hypothyroid, rheumatoid arthritis (and other “arthropathies”), taking birth control pills (BCPs), and more can cause CTS without any increase in hand/wrist activities!
So HOW can we prevent CTS?
First, consider your job and your “workstation.” There are ergonomic keyboard and mouse options that can help you maintain a “neutral” wrist posture. If you have to bend your wrist a lot to do your work tasks—like placing items in a package, assembly work, etc.—see if you can change the angle of the package or assembly set up that allows your wrist to be straight, NOT BENT! Also, sit/stand up straight, chin tucked back, and DON’T SLOUCH!
A “night splint” forces the wrist to stay straight and can REALLY help! Managing your weight and health (manage your diabetes, thyroid, and medications that increase swelling like BCPs) is VERY important! There are also natural anti-inflammatory vitamins and herbs like ginger, turmeric, and bioflavonoid you may want to consider—your doctor of chiropractic can help you with this!
Chiropractors can manage CTS very well and can frequently help patients avoid the need for a surgical release. The “KEY” is to not wait—get treated early on!