Since 2005, Bryan has been dedicated to helping all people with chronic and acute pain caused by soft-tissue damage.
His training and experience make him uniquely qualified to treat a wide variety of pain and dysfunction and to give instruction on prevention and self-care.
Bryan is the only Massage Therapist in Manitoba — and one of the few in Canada — to be certified by the Certification Board for Myofascial Trigger Point Therapists (CBMTPT).
Bryan holds a degree as an Advanced Remedial Massage Therapist (ARMT) from the Massage Therapy College of Manitoba. Course work at MTCM includes
• over 2,000 hours of practice, as well as
• intensive course work,
• a supervised clinical practicum, and
• community outreach placements.MTCM has a credit transfer affiliation with the University of Winnipeg, ensuring that its courses are held to the highest level. When Bryan studied at MTCM, the college was the only massage therapy college in western Canada accredited by the Commission on Massage Therapy Accreditation. Today, the college is a member of the Canadian Council of Massage Therapy Schools.
Bryan is a member in good standing of the Natural Health Practitioners of Canada.
Bryan also has a background in Anatomy, Exercise Physiology, and Sport Sciences from the University of Manitoba, and he has worked as a personal trainer and fitness leader.
He is an avid natural bodybuilder and fitness enthusiast, and has a blue belt in Brazilian jiu-jitsu.
Migrane
Trigger points in the temporalis muscle
The temporalis muscle is located in the temple area of the skull. It originates on the temporal lines on the parietal bone of the skull, and inserts on the coronoid process of the mandible. It’s main action is to close the jaw. The posterior and middle fibres bilaterally retrude the mandible. Acting individually, this muscle will deviate the mandible to the same side. Trigger points in this muscle refer into the teeth causing hypersensitivity, and into and above the eye and temple, causing headaches.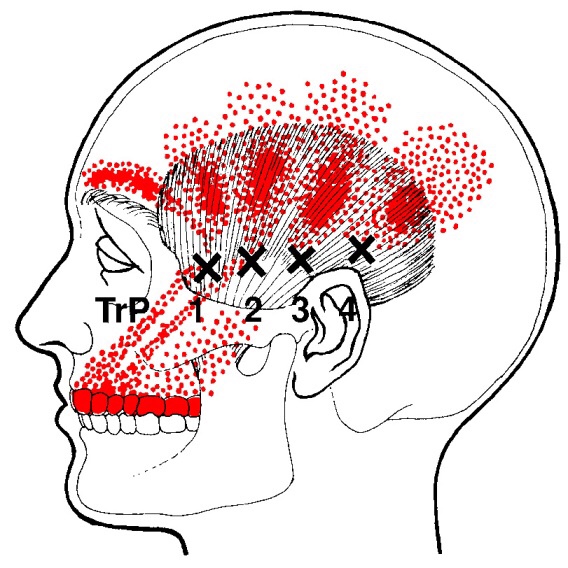
Can Chiro help me?

Chiropractic is the most widely accepted and most frequently used type of “alternative” healthcare in the United States. This is largely due to the fact that it works, and because of that, there has been a steady increase in acceptance by the public, third-party payers, and the Federal government. Since the mid-1990s, a number of outside (non-chiropractic) observers have suggested that chiropractic has now entered mainstream healthcare.
One can position chiropractic as being BOTH alternative and mainstream. It is “alternative” since it approaches healthcare from an entirely different direction compared to the primary care medical profession. Chiropractic is non-surgical and promotes diet and nutritional approaches vs. drugs and surgery. Chiropractic is also arguably “mainstream” as it has evolved into a strongly utilized form of primary care through popular acceptance and utilization by the public.
So, what role does chiropractic play in today’s health delivery system? This question is still being debated, but there appears to be three camps: 1) Specialist—limited to musculoskeletal (MSK) complaints on an interdisciplinary primary healthcare team; 2) Primary healthcare “gatekeepers” that focus on ambulatory MSK complaints; 3) Generalist primary healthcare provider of “alternative or complementary” medicine that manage and/or co-manage both MSK AND non-MSK conditions.
Looking at this from the patient or “consumer” perspective, chiropractic already plays an important role in the healthcare delivery for many patients. In 1993, a report claimed 7% of American adults had received chiropractic care during the prior year. According to a 2015 Gallup poll (that included 5,442 adults, aged 18+, surveyed between 2/16/15 and 5/6/15) entitled, Majority in U.S. Say Chiropractic Works for Neck, Back Pain, “Chiropractic care has a positive reputation among many US adults for effective treatment of neck and back pain, with about six in 10 adults either strongly agreeing (23%) or agreeing somewhat (38%) that chiropractors are effective at treating these types of pain.”
The “highlights” from this Gallup poll include: 1) Two-thirds say chiropractic is effective for neck and back pain. 2) Many adults say chiropractors think of the patient’s best interest. 3) More than 33 million adults in the United States (US) saw a chiropractor in the twelve months before the survey was conducted. That means roughly 14% of U.S. adults saw a chiropractor in the 12 months prior to the survey (vs. 7% in 1993). An additional 12% who responded to the Gallup pollsters saw a chiropractor in the last five years but not in the last 12 months. Overall, 51% of those polled had previously seen a chiropractor.
Whether or not you have personally utilized chiropractic, the educational process, licensing requirements, public interest, third-party payer systems, and interprofessional cooperation ALL support firm ground for which you can comfortably and confidently seek chiropractic care for your complaints.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care, we would be honored to render our services.
Pathophysiology of trigger points.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
Diagnosis of trigger points.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
What is a trigger point
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
Trigger points in the trapezius muscle.
The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
Trigger points in the Levator scapula
The Levator scapula is a muscle in your neck that originates on the transverse processes of C1-C4 and inserts on the superior part of the medial border of the scapula. The primary actions of this muscle are to elevate the scapula and rotate the glenoid fossa downward. It also rotates the neck to the same side and assists in extension. When this muscle is tight it restricts neck rotation resulting in the classic “stiff neck”. With a forward head position the Levator is often stretched and over worked. To help combat this you must get the head back by releasing the anterior chest and neck muscles. Trigger points in this muscle refer pain into the angle of the neck and down the shoulder blade.
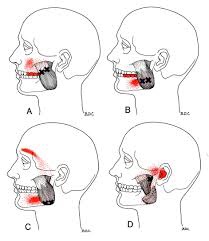
Trigger points in the masseter muscle

The masseter is the main muscle that moves your jaw. It originates on the zygomatic arch and maxilla, and inserts on the coronoid process and Ramus of the mandible. It’s actions are to elevate the mandible and close the jaw. The deep fibres of this muscle also retrude the mandible. This muscle commonly harbours trigger points as a result of teeth grinding. Trigger points in this muscle are often also associated with tmj dysfunction. Trigger points in the upper part of this muscle will refer pain to the upper molars and maxilla often felt as sinusitis. Trigger points in the lower portion of this muscle refer to the lower molars and temple. All trigger points can cause tooth sensitivity