The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.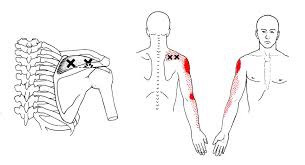
Massage Therapy
Trigger points in the infraspinatus
The infraspinatus muscle is one of the muscles that makes up the rotator cuff. It originates on the infraspinous fossa of the scapula, and inserts on the middle facet of the greater tubercle of the humerus. It functions to externally rotate the humerus and to stabilize the head of the humerus in the glenoid cavity during upward movement of the arm. Trigger points in this muscle refer pain deep into the anterior shoulder joint and down the anterior arm. Trigger points near the lower medial border refer pain into the rhomboids. This muscle is often injured during throwing motions.
Trigger points in the triceps muscle.
The tricep muscle is named for its three heads long, medial, and lateral. The long head originates on the infraglenoid tubercle, the medial head on the posterior humerus, and the lateral head on the posterior humerus as well. They join together to insert on the Olecranon process of the ulna. The triceps function to extend the elbow. Strong extension under resistance can cause trigger points to form. Pain referred from triceps trigger points can be felt in the posterior shoulder and down the posterior forearm, as well as in in the olecranon process and the lateral epicondyle which can cause “tennis elbow” pain.
Pathophysiology of trigger points.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
Diagnosis of trigger points.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
Trigger points in the biceps Brachii muscle.
The Bicep Brachii is perhaps the most recognizable muscle in the body. It’s the muscle that is most often flexed when someone says ” show me your muscles”. It is composed of two heads, the long head and the short head. The short head originates on the coracoid process of the scapula, and the long head on the supraglenoid tubercle. Both heads merge to insert on the radial tuberosity and bicipital aponeurosis into the deep fascia on the medial part of the forearm. The main actions of this muscle are elbow flexion and forearm supination(rotation with the palm of the hand going upward). This muscle also assists shoulder flexion. Trigger points in this muscle mainly refer pain into the shoulder, with spillover into the posterior aspect above the scapula. A less common referral is into the anterior elbow and forearm. 
What is a trigger point
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
Trigger points in the deltoid muscle.
The deltoid is the the muscle that is most often thought of as the “shoulder.” It is the diamond shaped muscle that caps the shoulder joint. It originates on the clavicle, the acromion, and the spine of the scapula. It inserts on the deltoid tuberosity of the humerus. As a whole unit the deltoid laterally abducts the humerus at the glenohumeral joint. The anterior portion of the delt forward flexes the arm, as well as horizontally flexing the arm across the chest. Since the deltoid is involved in almost all shoulder movements it is especially prone to trigger points. Points in the anterior deltoid refer into the anterior and lateral shoulder. Trigger points in the posterior deltoid refer pain into the posterior shoulder with spillover down the lateral arm. 
Trigger points in the pectoralis minor muscle.
The pectoralis minor is a small strap like muscle that is underneath (deep) to the pectoralis major. It originates on the third to fifth rib, near the costal cartilages. It’s insertion is on the coracoid process of the scapula. It acts to draw the scapula forward, downward, and inward at nearly equal angles ( think of rounding or shrugging your shoulders forward). This muscle is very often shortened and tight in people due to the high prevalence of desk jobs. This muscle pulls the shoulder blade forward resulting in the muscles in the back(rhomboid and mid traps) being chronically strained. Trigger points that form in the pec minor primarily refer pain over the anterior chest and shoulder, with spillover down the medial arm. Trigger points in the left side can mimic angina. 
