The muscles of the hip provide not only local stability, but also play an important role in spinal and lower extremity functional alignment. (1-4) While weakness in some hip muscles (hip extensors and knee extensors) is well tolerated, weakness or imbalance in others can have a profound effect on gait and biomechanical function throughout the lower half of the body. (5) Weakness of the hip abductors, particularly those that assist with external rotation, has the most significant impact on hip and lower extremity stability. (5,6)

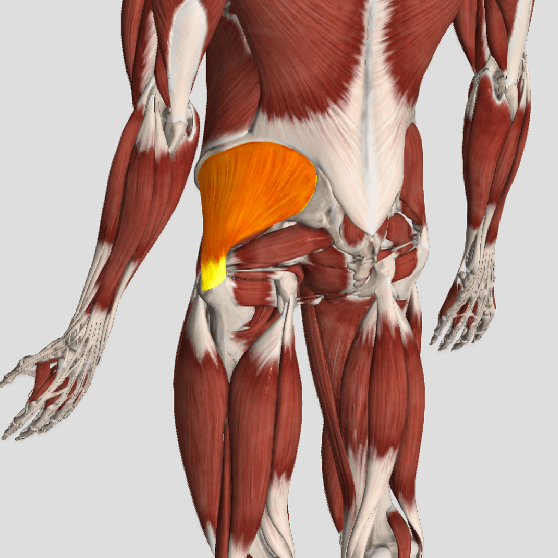
The gluteus medius is the principal hip abductor. When the hip is flexed, the muscle also assists the six deep hip external rotators (piriformis, gemelli, obturators, and quadratus femoris). The gluteus medius originates on the ilium just inferior to the iliac crest and inserts on the lateral and superior aspects of the greater trochanter. While the principal declared action of the gluteus medius is hip abduction, clinicians will appreciate its more valuable contribution as a dynamic stabilizer of the hip and pelvis- particularly during single leg stance activities like walking, running, and squatting. The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance. The remainder comes predominantly from 2 muscles that insert onto the iliotibial band: the tensor fascia lata and upper gluteus maximus. Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity. (6)
Incompetent hip abductors and/or external rotators allows for excessive adduction and internal rotation of the thigh during single leg stance activities. This leads to a cascade of biomechanical problems, including pelvic drop, excessive hip adduction, excessive femoral internal rotation, valgus knee stress, and internal tibial rotation. (1,7-12)
References
1. Szu-Ping Lee, Powers C. Description of a Weight-Bearing Method to Assess Hip Abductor and External Rotator Muscle Performance. JOSPT. Volume 43, Issue 6
2. Crossley KM, Zhang WJ, Schache AG, Bryant A, Cowan SM. Performance on the single-leg squat task indicates hip abductor muscle function. Am J Sports Med. 2011;39:866-873.
3. Presswood L, Cronin J, Keogh JWL, Whatman C. Gluteus medius: applied anatomy, dysfunction, assessment, and progressive strengthening. Strength Cond J. 2008;30:41-53.
4. Sled EA, Khoja L, Deluzio KJ, Olney SJ, Culham EG. Effect of a home program of hip abductor ex- ercises on knee joint loading, strength, function, and pain in people with knee osteoarthritis: a clinical trial. Phys Ther. 2010;90:895-904.
5. van der Krogt MM, Delp SL, Schwartz MH How robust is human gait to muscle weakness? Gait Posture. 2012 Feb 29.
6. Laurie Stickler, Margaret Finley, Heather Gulgin Relationship between hip and core strength and frontal plane alignment during a single leg squat Physical Therapy in Sport Available online 2 June 2014
7. Ireland ML, Willson JD, Ballantyne BT, Davis
IM. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33:671-676.
8. Noehren B, Davis I, Hamill J. ASB clinical biome- chanics award winner 2006: prospective study of the biomechanical factors associated with iliotib- ial band syndrome. Clin Biomech (Bristol, Avon). 2007;22:951-956.
9. Powers CM. The influence of abnormal hip me- chanics on knee injury: a biomechanical perspec- tive. J Orthop Sports Phys Ther. 2010;40:42-51.
10. Powers CM. The influence of altered lower- extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther. 2003;33:639-646.
11. Sigward SM, Powers CM. Loading characteristics of females exhibiting excessive valgus moments during cutting. Clin Biomech (Bristol, Avon). 2007;22:827-833
12. Souza RB, Powers CM. Differences in hip kine- matics, muscle strength, and muscle activation between subjects with and without patellofemo- ral pain. J Orthop Sports Phys Ther. 2009;39:12- 19.