Since 2005, Bryan has been dedicated to helping all people with chronic and acute pain caused by soft-tissue damage.
His training and experience make him uniquely qualified to treat a wide variety of pain and dysfunction and to give instruction on prevention and self-care.
Bryan is the only Massage Therapist in Manitoba — and one of the few in Canada — to be certified by the Certification Board for Myofascial Trigger Point Therapists (CBMTPT).
Bryan holds a degree as an Advanced Remedial Massage Therapist (ARMT) from the Massage Therapy College of Manitoba. Course work at MTCM includes
• over 2,000 hours of practice, as well as
• intensive course work,
• a supervised clinical practicum, and
• community outreach placements.MTCM has a credit transfer affiliation with the University of Winnipeg, ensuring that its courses are held to the highest level. When Bryan studied at MTCM, the college was the only massage therapy college in western Canada accredited by the Commission on Massage Therapy Accreditation. Today, the college is a member of the Canadian Council of Massage Therapy Schools.
Bryan is a member in good standing of the Natural Health Practitioners of Canada.
Bryan also has a background in Anatomy, Exercise Physiology, and Sport Sciences from the University of Manitoba, and he has worked as a personal trainer and fitness leader.
He is an avid natural bodybuilder and fitness enthusiast, and has a blue belt in Brazilian jiu-jitsu.
Healthy Living
Trigger points in the Quadratus Lumborum muscle.
The quadratus lumborum muscle is a commonly overlooked source of low back pain and is often responsible for “pseudo disc syndrome”. This muscle originates on the inferior border of the 12th rib and lumbar transverse processes. It inserts on the iliac crest and iliolumbar ligament. The q.l.’s main actions are extension and lateral flexion of the spine. It also acts as a stabilizer of the lumbar spine. Trigger points in this muscle refer pain into the sacroiliac joint and the lower buttock. Pain can also spread anteriorly along the crest of the ilium into the lower abdomen and groin and to the greater trochanter. 
Trigger points in the temporalis muscle
The temporalis muscle is located in the temple area of the skull. It originates on the temporal lines on the parietal bone of the skull, and inserts on the coronoid process of the mandible. It’s main action is to close the jaw. The posterior and middle fibres bilaterally retrude the mandible. Acting individually, this muscle will deviate the mandible to the same side. Trigger points in this muscle refer into the teeth causing hypersensitivity, and into and above the eye and temple, causing headaches.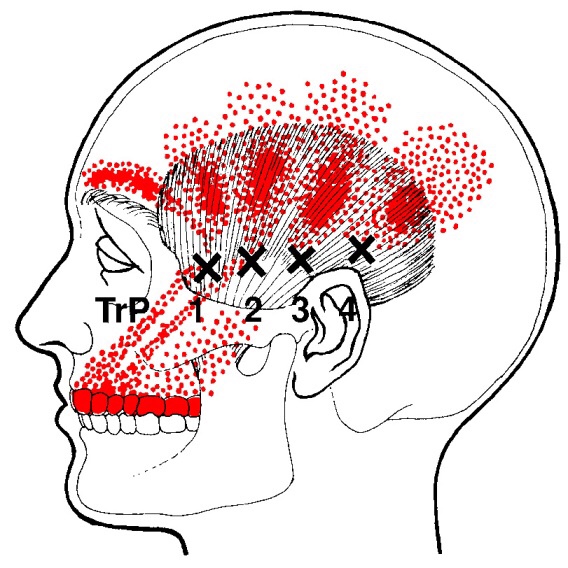
Do you wake up with numb fingers?
The term “thoracic outlet” describes an area at the base of your neck, just above your collarbone. Some important nerves and vessels pass through this outlet on their way into your arm. Compression of these tissues causes a condition called “thoracic outlet syndrome” which results in pain, numbness or tingling in your arm.
Several different factors can cause Thoracic Outlet Syndrome,

commonly referred to as TOS. Sometimes TOS is caused from tightness in the muscles of your neck and chest, other times the space between your first rib and collarbone is too small. People who have an extra rib (cervical rib) and people who have recently suffered a neck injury may have a greater chance of having this problem.
The condition is aggravated by poor posture and by occupations that promote “slouching,” i.e., computer users, assembly line workers, supermarket checkers and students. Swimmers, volleyball players, tennis players, baseball pitchers and occupations requiring prolonged overhead activity. i.e., electricians and painters are also prime candidates for TOS.
Symptoms of TOS include arm pain, numbness, tingling and possible weakness. Neck, arm and hand pain may begin slowly and are often aggravated by elevation of the arms or excessive head movement. Loss of grip strength is possible.
Conservative treatment, like the kind we provide, has been shown to be effective at treating TOS. Through our careful exam we have identified your specific sites of compression and will use some of the following treatment to help:
You should avoid carrying heavy loads, especially on your shoulder i.e., carpet rolls. Briefcases, laptop cases or heavy shoulder bags should be lightened. Bra straps may need additional padding or consideration of replacement with a sports bra.
Trigger points in the lateral pterygoid
The lateral pterygoid muscle plays an important role in prober jaw function. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate, and inserts on the condyloid process of the mandible. It’s action is to pull the head of the mandibular condyle out of the mandibular fossa while opening the jaw. When trigger points develop they refer pain into the temporal mandibular joint and maxillary sinus. This referral is commonly mistaken for TM arthritis. In addition to the referral pain, trigger points in this muscle can also effect proper movement of the jaw.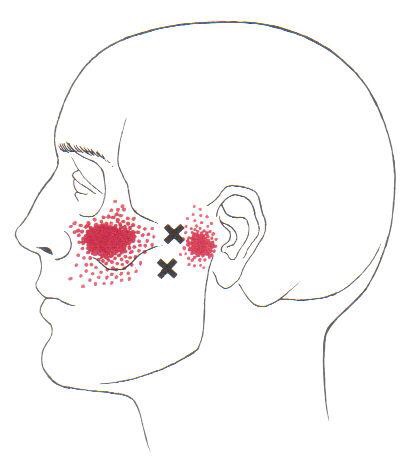

Trigger points in the serratus anterior
The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.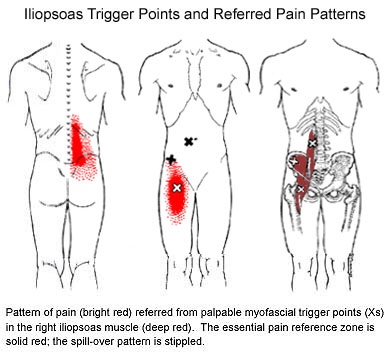
What is Fibromyalgia?
Fibromyalgia, although often misdiagnosed and misunderstood, is the second most common musculoskeletal disorder behind osteoarthritis. The condition affects nearly 12 million Americans and is ten times more common in women.
The diagnosis of fibromyalgia is made when a certain set of symptoms has been present for at least three months. The most common symptoms include wide-spread muscle and joint pain, achiness or soreness- especially in the neck, shoulders, back, and hips. Your muscles may constantly feel overworked and tired. Fibromyalgia patients often exhibit a set of predictable “tender points” spread throughout the body. Some patients have trouble sleeping and feel as though they are in a “brain fog” most of the day. This can lead to fatigue or mood changes, like anxiety and depression.

Stress is a known contributor to fibromyalgia, and patients should seek ways to de-stress, including yoga or meditation. Fibromyalgia patients should minimize their caffeine intake, as this is a known stimulant for nervousness, anxiety, and insomnia. Breathing exercises are sometimes helpful.
Although your sleep may be restless, you should try to establish a bedtime routine that gives your body the best chance for recovery. Try to avoid late night electronics, like the television or computer. Keep your bedroom dark, quiet, cool, and distraction-free. Be sure to take time for yourself each day for relaxation or to do something you enjoy. Combat “brain fog” by carrying a notebook or a phone to make notes for important things. Some patients report decreased muscle tightness by applying moist heat or a taking warm bath. The American Pain Society recommends conservative treatment, including chiropractic, along with moderate aerobic exercise.
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 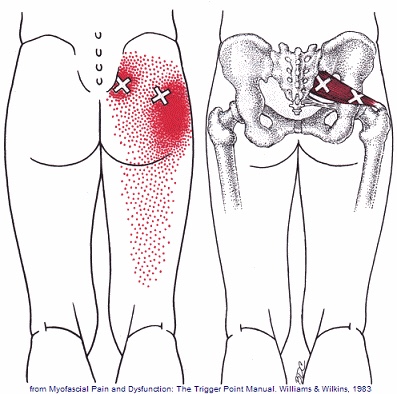
Osteoporosis and Compression Fractures
Most of the tissues in our body are in a constant state of rejuvenation, wherein old cells are removed to be replaced by new. In our skeleton, when the production of new bone cannot keep up with the rate of tear down, our bones become progressively thinner and weaker in a process called “osteoporosis”.

Bone fractures occur when stress to a bone exceeds the bone’s ability to support that load. In healthy vertebrae, significant stress is required to cause a fracture. But in osteoporotic bones, the threshold for injury is lowered to the point that “compression fractures” may occur with seemingly minimal stress like bending, coughing, or sneezing. A compression fracture causes a wedge-shaped collapse of the front of the vertebral “body”- resembling what would occur after stepping on one edge of an aluminum can.
Compression fractures are two to three times more common in women, and the risk of developing the problem increases over time. People who have had a prior compression fracture are at greater risk for developing a subsequent fracture. Additional risk factors for compression fracture include a family history of osteoporosis, low body weight, recent weight loss, smoking, a sedentary lifestyle, poor dietary choices, inadequate calcium or vitamin D intake, excessive alcohol or caffeine intake, and scoliosis. The American Academy of Orthopedic Surgery recommends bone density screening for osteoporosis in all women over age 65 or post-menopausal women who have suffered a compression fracture. If you have not already done so, you should schedule a bone density screening.
Symptoms of a compression fracture include an “aching” or “stabbing” pain in the back, near the site of fracture. Symptoms can range from minimal to disabling. Often times, pain is referred to the ribs, hip, groin, or buttocks. Be sure to tell your doctor if you have pain or numbness that radiates into your legs, weakness, clumsiness, loss of bowel or bladder control, impotence, fever, unexplained weight loss, night sweats, excessive fatigue, or a history of cancer.
Symptoms from a compression fracture typically lasts for six to 12 weeks. Occasionally, patients will require surgical treatment of a compression fracture, but fortunately, most respond to conservative care. In general, you should maintain a relatively active lifestyle and try to avoid bed rest. If your pain prevents movement, you may talk to your doctor about wearing a brace to limit stress.
Our office will prescribe exercises to help you recover and reduce the risk of subsequent fracture. As your symptoms improve, you can begin incorporating some aerobic exercise, like walking on a treadmill. Studies have shown that light resistance training (i.e. weights and elastic bands) may help you maintain bone density and reduce the risk of future fractures. Supplements to help manage osteoporosis include daily intake of 800-1000 IU of vitamin D and 1000-1200 mg of calcium.
