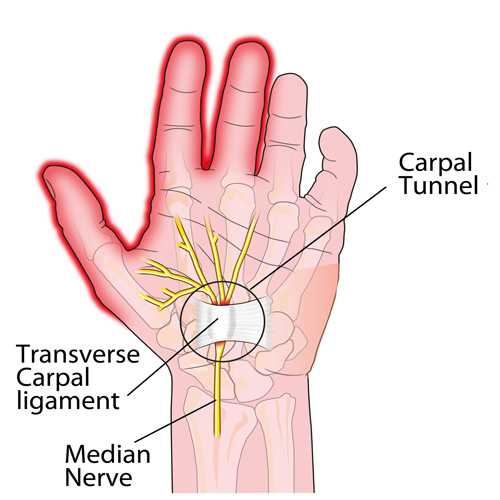
Carpal tunnel syndrome (CTS) is a very common condition. According to a report by the Bureau of Labor Statistics (BLS), CTS ranks SECOND among the major disabling diseases and illnesses in ALL private industries. The BLS states that workers with CTS may eventually have to give up their livelihood. They cite one study in which almost half of all CTS patients changed their jobs within 30 months following their diagnosis. Due to the controversy surrounding the issue of CTS and worker’s compensation, workers do not always receive compensation benefits.
The KEY to long-term cost containment associated with CTS is EARLY DIAGNOSIS and PREVENTION! The challenge is getting the worker to identify early symptoms and NOT feel intimidated to report them, which could then lead to prompt care and possibly job modifications, resulting in the best chance of preventing a more complicated and far more costly problem.
Because of the many factors that contribute to and/or cause CTS, there is similarly no one way to prevent it from happening. Treating any/all underlying medical condition(s) is important. Using simple common sense can go a long way to help minimize some of the risk factors that predispose a person to work-related CTS and other cumulative trauma disorders (CTDs).
For example, watching and mimicking veteran workers can be a great guide as to how to maximize efficient work methods while minimizing unnecessary stresses and strains. Other preventative “tricks” include learning how to adjust the work area, handle tools, or perform tasks that minimize hand/wrist strain. Maintaining proper posture and exercise programs to strengthen the fingers, hands, wrists, forearms, shoulders, and neck may also help prevent CTS.
Many companies have taken action to help prevent repetitive stress injuries. In one study, 84% of the companies surveyed reported that they were modifying equipment, tasks, and processes as part of a prevention effort; nearly 85% analyzed their workstations and jobs; and 79% purchased more ergonomic equipment. Unfortunately, there is NO EVIDENCE that any of these methods can completely protect a worker against CTS. Often, the best approach is to relocate the worker to a less repetitive job, but this is not always an option.
Doctors of chiropractic can observe the worker through a video or during a factory tour/visit and often identify ergonomic problems that can result in a low-cost, easy modification. Simple modifications coupled with quality care, patient education, and cooperation from BOTH the worker and the employer can typically help yield the best outcome for the CTS patient.