The temporalis muscle is located in the temple area of the skull. It originates on the temporal lines on the parietal bone of the skull, and inserts on the coronoid process of the mandible. It’s main action is to close the jaw. The posterior and middle fibres bilaterally retrude the mandible. Acting individually, this muscle will deviate the mandible to the same side. Trigger points in this muscle refer into the teeth causing hypersensitivity, and into and above the eye and temple, causing headaches.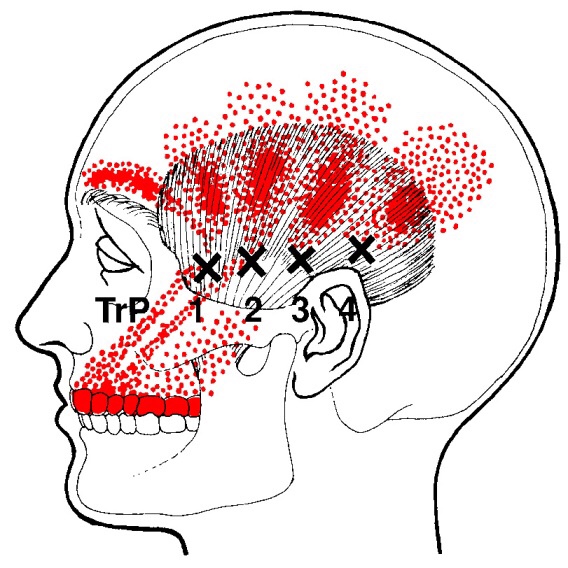
Headache
Trigger points in the lateral pterygoid
The lateral pterygoid muscle plays an important role in prober jaw function. It originates on the greater wing of the sphenoid bone and the lateral pterygoid plate, and inserts on the condyloid process of the mandible. It’s action is to pull the head of the mandibular condyle out of the mandibular fossa while opening the jaw. When trigger points develop they refer pain into the temporal mandibular joint and maxillary sinus. This referral is commonly mistaken for TM arthritis. In addition to the referral pain, trigger points in this muscle can also effect proper movement of the jaw.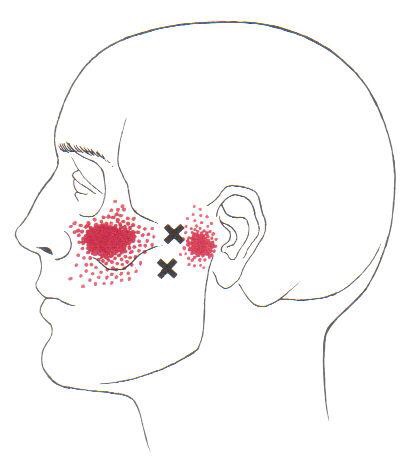

Can Chiro help me?

Chiropractic is the most widely accepted and most frequently used type of “alternative” healthcare in the United States. This is largely due to the fact that it works, and because of that, there has been a steady increase in acceptance by the public, third-party payers, and the Federal government. Since the mid-1990s, a number of outside (non-chiropractic) observers have suggested that chiropractic has now entered mainstream healthcare.
One can position chiropractic as being BOTH alternative and mainstream. It is “alternative” since it approaches healthcare from an entirely different direction compared to the primary care medical profession. Chiropractic is non-surgical and promotes diet and nutritional approaches vs. drugs and surgery. Chiropractic is also arguably “mainstream” as it has evolved into a strongly utilized form of primary care through popular acceptance and utilization by the public.
So, what role does chiropractic play in today’s health delivery system? This question is still being debated, but there appears to be three camps: 1) Specialist—limited to musculoskeletal (MSK) complaints on an interdisciplinary primary healthcare team; 2) Primary healthcare “gatekeepers” that focus on ambulatory MSK complaints; 3) Generalist primary healthcare provider of “alternative or complementary” medicine that manage and/or co-manage both MSK AND non-MSK conditions.
Looking at this from the patient or “consumer” perspective, chiropractic already plays an important role in the healthcare delivery for many patients. In 1993, a report claimed 7% of American adults had received chiropractic care during the prior year. According to a 2015 Gallup poll (that included 5,442 adults, aged 18+, surveyed between 2/16/15 and 5/6/15) entitled, Majority in U.S. Say Chiropractic Works for Neck, Back Pain, “Chiropractic care has a positive reputation among many US adults for effective treatment of neck and back pain, with about six in 10 adults either strongly agreeing (23%) or agreeing somewhat (38%) that chiropractors are effective at treating these types of pain.”
The “highlights” from this Gallup poll include: 1) Two-thirds say chiropractic is effective for neck and back pain. 2) Many adults say chiropractors think of the patient’s best interest. 3) More than 33 million adults in the United States (US) saw a chiropractor in the twelve months before the survey was conducted. That means roughly 14% of U.S. adults saw a chiropractor in the 12 months prior to the survey (vs. 7% in 1993). An additional 12% who responded to the Gallup pollsters saw a chiropractor in the last five years but not in the last 12 months. Overall, 51% of those polled had previously seen a chiropractor.
Whether or not you have personally utilized chiropractic, the educational process, licensing requirements, public interest, third-party payer systems, and interprofessional cooperation ALL support firm ground for which you can comfortably and confidently seek chiropractic care for your complaints.
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care, we would be honored to render our services.
Work Station Ergonomics Advice
When dealing with Upper Crossed Syndrome the ergonomics of your workstation should be at the from of mind. Some workstation ergonomics advice is as follows:
✓ Maintain proper body position and alignment while sitting at your desk – Hips, knees and elbows at 90 degrees, shoulders relaxed, feet flat on floor or footrest.
✓ Wrists should not be bent while at the keyboard. Forearms and wrists should not be leaning on a hard edge.
✓ Use audio equipment that keeps you from bending your neck (i.e., Bluetooth, speakerphones, headsets).
✓ Monitors should be visible without leaning or straining and the top line of type should be 15 degrees below eye level.
✓ Use a lumber roll for lower back support.
✓ Avoid sitting on anything that would create an imbalance or uneven pressure (like your wallet).
✓ Take a 10-second break every 20 minutes: Micro activities include: standing, walking, or moving your head in a “plus sign” fashion.
✓ Periodically, perform the “Brugger relief position” -Position your body at the chair’s edge, feet pointed outward. Weight should be on your legs and your abdomen should be relaxed. Tilt your pelvis forward, lift your sternum, arch your back, drop your arms, and roll out your palms while squeezing your shoulders together. Take a few deep cleansing breaths.
Addressing these areas will help reduce your symptoms, make your care more effective and the duration of pain decrease. If you need help with ergonomics or want more information, please contact us at info@aberdeenchiropratcic.com
Pathophysiology of trigger points.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
Upper Crossed Syndrome/Desk Neck

Your posture plays an important role in your overall health. Poor posture leads to chronic strain and discomfort. “Upper crossed syndrome” describes poor posture that results from excessive tightness in your shoulders and chest with weakness in your neck and mid-back. This combination forces your shoulders to roll inward and your head to project forward.
To help understand how upper crossed syndrome causes trouble, think of your spine as a telephone pole and your head as a bowling ball that sits on top. When the bowling ball is positioned directly over the top of the upright post, very little effort is required to keep it in place. If you tip the post forward and the ball begins to roll over the edge of the post, significantly more effort would be required from the muscles trying to hold it there. This effort results in chronic strain of the muscles of your neck and upper back.
The chronic strain is uncomfortable and may also lead to neck pain, upper back pain, headaches, TMJ pain, and ultimately- arthritis. This postural problem is exceptionally common in computer workstation users.
Correction of this problem is accomplished by stretching the tight muscles, strengthening weak muscles, and modifying your workstation. Treatment is aimed at reducing and eliminating symptoms through the use of Chiropractic adjustments, soft tissue release, acupuncture and trigger point therapy.
Diagnosis of trigger points.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
What is a trigger point
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
He barely hit me; why does it hurt?
Error
This video doesn’t exist
You may have heard the comment, “If there’s no damage to the car, then there’s no injury.” Unfortunately, that does not always seem to be the case.
There are MANY factors that affect the dynamics of a collision and whether or not injury occurs. A short list includes: vehicle type and design, speed, angle of collision, momentum, acceleration factors, friction, kinetic and potential energy, height, weight, muscle mass, seat back angle and spring, head position upon impact, etc.
Consider Sir Isaac Newton’s Third Law of Motion: “For every action there is an equal and opposite reaction.” This law applies to a car accident at any speed. Using the analogy of hitting a pool ball into the corner pocket straight on, when the cue ball stops, its momentum is transferred to the target ball which accelerates at the same speed…hopefully into the corner pocket!
This example is not quite the same as an automobile collision because the energy transfer is very efficient due in part to the two pool balls not deforming (crushing or breaking) on impact with one another. If either ball did deform, more energy absorption would occur and the acceleration of the second ball would be lower.
In fact, in the United States, vehicle bumpers are tested at 2.5 mph with impact equipment of similar mass with the test vehicle’s brakes disengaged and the transmission in neutral. National Highway Transportation Highway Safety Administration (NHTSA) vehicle safety standards demand that no damage should occur to the car in this scenario.
However, energy transfer occurs very quickly and with a greater amount of force when there is no vehicle deformation (damage). As a result, a greater amount of energy (described as G-force) is directly transferred to the occupants inside the vehicle—increasing the risk of injury. A 1997 Society of Automobile Engineers article provided an example in which the same 25 mph (12 m/s) collision resulted in a five-times greater force on the occupants of the vehicle when the crush distance of the impact fell from 1 meter to .2 meters.
So be aware that even low-speed impacts can still place quite a bit of force on your body, even if the bumper of your car doesn’t have a scratch on it.
