The gluteus minimus is a small but important muscle that lies deep to the gluteus medius. It originates on the gluteal surface of the ilium, and attaches on the greater trochanter of the femur. It’s main actions are to abduct and medically rotate the hip. Trigger points in this muscle refer pain into the buttock and down the lateral and posterior leg, mimicking sciatica. This muscle should be the first to be examined if a straight leg test turns out negative. 
Fitness
Trigger points in the gluteus medius muscle
The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
Achilles Tendonitis: The Details
Your Achilles tendon is the strong fibrous band of tissue that connects your calf muscles to your heel. The tendon is named after “Achilles” who was a powerful, yet vulnerable warrior in Greek mythology. Likewise, our Achilles tendon, being the largest and strongest tendon in the body, is susceptible to injury from the high demands placed on it. (Running can generate forces over 12 times your bo

dy weight on the Achilles tendon.)
The tendon may be strained or even ruptured from excessive stretch or forceful contraction of the calf muscles. More commonly, the tendon is repeatedly overloaded and suffers tiny “micro tears.” Damage usually occurs either directly behind the heel, or near the weakest area of the tendon- one to two inches above the heel.
Achilles tendon injuries affect between 250,000 and 1 million people per year. Most are middle-aged males, between the age of 30 and 50. Interestingly, Achilles tendon injuries occur more frequently on the left side. If you have suffered a prior Achilles tendon injury, you are at greater risk of injuring the opposite side. Two-thirds of all Achilles tendon injuries involve athletes. Runners are up to 10 times more likely to suffer Achilles tendon problems. You may at increased risk if the arch of your foot is too high or too flat.
Symptoms may begin abruptly following a strain but more commonly develop slowly from repeated irritation. Morning pain and stiffness are common. Your symptoms will likely increase with activity, especially walking or running. You may notice pain when you rise up on your toes. Walking down stairs stretches the tendon and usually increases symptoms. Some patients notice that the irritated area becomes firmly swollen. Ongoing irritation to the spot on your heel where the tendon inserts can cause a painfully elevated “pump bump.”
Research has shown that conservative care, like the type provided in this office, can produce “excellent results” in over 85% of patients. Initially, you may need to limit or stop activities that cause pain. Runners may need to switch to swimming or cycling for a short period of time. Be sure to introduce new activities slowly and avoid increasing your activity by more than 10% per week. Runners should begin on a smooth, shock-absorbent surface and start at a low intensity – first increasing distance, then pace. Avoid training on hard or unlevel surfaces like hills. Make sure you warm up properly and avoid over training. Avoid wearing high heels or shoes with an excessively rigid heel tab. One of the most important and effective treatments for Achilles tendinopathy is performing “heel drop exercises” as outlined below.
Eccentric Achilles Strengthening
Begin standing up on your toes with the affected foot on the edge of a step. Do not place weight on your good leg, but you may use it for stability. Slowly lower your affected heel, at a count of 4 seconds, until you reach a fully stretched position and can drop no further. Use your good leg to return to your toes. Repeat 3 sets of 15 repetitions with your knee straight and 3 more sets of 15 repetitions with your knee slightly bent, twice daily or as directed. Moderate pain during this exercise is acceptable but if pain is excessive, you should assist downward motion with the non-injured leg.
Here is a brief description of the treatments we may use to help manage your problem.
 Joint Manipulation
Your chiropractor has found joints in your body that are not moving freely. This can cause tightness and discomfort and can accelerate unwanted degeneration i.e. arthritis. Your chiropractor will apply a gentle force with their hands, or with hand held instruments, in order to restore motion to any “restricted” joints. Sometimes a specialized table will be used to assist with these safe and effective “adjustments”. Joint manipulation improves flexibility, relieves pain and helps maintain healthy joints.
 Therapy Modalities
We may apply electrotherapy modalities that produce light electrical pulses transmitted through electrodes placed over your specific sites of concern. These comfortable modalities work to decrease your pain, limit inflammation and ease muscle spasm. Hot or cold packs are often used in conjunction, to enhance the effect of these modalities. Another available option is therapeutic ultrasound. Ultrasound pushes sound vibrations into tissues. When these vibrations reach your deep tissues, heat develops and unwanted waste products are dispersed.
 Myofascial Release
Overworked muscles often become tight and develop knots or “trigger points”. Chronic tightness produces inflammation and swelling that ultimately leads to the formation of “adhesions” between tissues. Your chiropractor will apply pressure with their hands, or with specialized tools, in order to release muscle tightness and soft-tissue adhesions. This will help to improve your circulation, relieve pain and restore flexibility.
 Therapeutic Exercise
Muscle tightness or weakness causes discomfort and alters normal joint function, leading to additional problems. Your chiropractor will target tight or weak muscles with specific therapeutic stretching and strengthening to help increase tissue flexibility, build strength, and ease pain. Healthy, strong, and flexible muscles may help prevent re-injury.
 Elastic Therapeutic Tape
Your chiropractor may apply a special elastic therapeutic tape in order to support injured areas or encourage better movement. This tape is thought to decrease pain and swelling, improve circulation and limit muscle soreness.
 Foot Evaluation
Fallen arches and faulty foot mechanics are common problems that can perpetuate your condition. Our office will carefully evaluate your feet and consider the need for a change in shoe style, arch supports or even custom orthotics.
 Ankle Brace
Our office may recommend using a support brace to protect your ankle from further injury. Your doctor will discuss the specific type of brace and provide instructions for use.
|
||
|
After this initial course of treatment we will reassess your progress. We will determine the need for any additional care after your reassessment.
|
||
Trigger points in the gluteus Maximus
The gluteus Maximus is the buttock muscle. It originates on the gluteal surface of the ilium, lumbar fascia, sacrum and sacrotuberous ligament. It inserts on the gluteal tuberosity of the femur and the iliotibial tract. Extension and lateral rotation of the hip are it’s main actions. This muscle is heavily involved in activities like ice skating and is a common area to develops trigger points. When trigger points do develop they can refer pain in a crescent pattern from the gluteal fold to the sacrum. Trigger points can also refer pain deep into the buttock itself making it feel like other deeper muscles are involved. These symptoms can sometimes be mistaken for s.i. Joint problems. 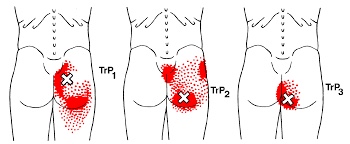
The Dreaded Lateral Ankle Sprain
“Ligaments” are made up of many individual fibers running parallel to each other and bundled to form a strong fibrous band. These fibrous bands hold your bones together. Just like a rope, when a ligament is stretched too far, it begins to fray or tear. “Sprain” is the term used to describe this tearing of ligament fibers.
Sprains are graded by the severity of damage to the ligament fibers. A Grade 1 sprain means the ligament has been painfully stretched, but no fibers have been torn. A Grade 2 sprain means some, but not all, of the ligaments’ fibers have been torn. A Grade 3 sprain means all of the ligaments’ fibers have been torn, and the ligament no longer has the ability to protect the joint.


Ankle sprains are the most common soft-tissue injury and will affect up to 20% of active people at some point in their life. Most ankle sprains occur because you have “rolled your ankle” inward. Sprains on the outer side of your ankle are much more common than sprains on the inner side. People who have suffered a prior ankle injury are more likely to suffer subsequent ankle injuries.
Ankle sprains cause pain and swelling over the outside of your ankle. Walking may be difficult, and bruising is common. Be sure to tell your doctor if you experience numbness, tingling, or a dramatic cold sensation in your foot, as this may indicate more significant injury.
Ankle sprains can be successfully managed but will require some work on your part. You can help reduce swelling by elevating your ankle by lying or sitting with your foot elevated or by using an ACE wrap for compression. Applying ice or ice massage for 10 minutes each hour may help relieve swelling. Depending upon the severity of your sprain, you may need to wear an ankle brace to help protect you from further injury. If walking is painful, crutches may be necessary.
Initially, a period of rest may be necessary in order to help you heal. Mild Grade 1 sprains may allow return to sport in a couple of days, while more severe injuries may take six weeks or longer to recover. Surgery is rarely necessary.
Trigger points in the infraspinatus
The infraspinatus muscle is one of the muscles that makes up the rotator cuff. It originates on the infraspinous fossa of the scapula, and inserts on the middle facet of the greater tubercle of the humerus. It functions to externally rotate the humerus and to stabilize the head of the humerus in the glenoid cavity during upward movement of the arm. Trigger points in this muscle refer pain deep into the anterior shoulder joint and down the anterior arm. Trigger points near the lower medial border refer pain into the rhomboids. This muscle is often injured during throwing motions.
Is there an actual cure all?

No; but exercise seems to be as close as we will ever get!
Some of you may have heard about how a modified form of boxing is helping patients with Parkinson’s disease (PD). If you haven’t, it’s been observed that people with Parkinson’s disease (PD) who engage in this boxing-like exercise routine can enhance their quality of life and even build impressive gains in posture, strength, flexibility, and speed. Proponents of the program report that regardless the degree of severity of PD, participants have a happier, healthier, and higher quality of life.
But must it be boxing? Maybe not. A report presented at the International Congress of Parkinson’s Disease and Movement Disorders in San Diego in June 2015 found that patients with Parkinson’s disease who began regular exercise early into the PD process had a much slower decline in their quality of life when compared with those who started exercising later. The researchers found just 2.5 hours per week of exercise is needed to improve quality of life scores. According to the report, it didn’t matter what exercise the participants did — simply getting up and moving for a total of 2.5 hours/week was reportedly enough (that’s only 20-25 minutes / day)!
Looking beyond Parkinson’s, other chronic conditions also benefit from adding exercise into a person’s lifestyle. Studies show that regular exercise as simple as walking helps reduce one’s risk for memory loss, and it slows down functional decline in the elderly. Incorporating aerobic exercise into one’s lifestyle can also improve reaction time in people at ALL AGES. Exercise has also been shown to improve both physical and emotional well-being in those afflicted with Alzheimer’s disease with as little as 60 minutes/week of moderate exercise! Patients with multiple sclerosis (MS) have also reported less stiffness and less muscle wasting when using exercise machines, aquatic exercise, and/or walking.
Research has shown just 30 minutes of brisk exercise three times a week can help reduce depressive symptoms in patients with mild-to-moderate depression. In a study involving teenagers, those who engaged in sports reported a greater level of well-being than their sedentary peers, and the more vigorous the exercise, the better their emotion health! In kids 8-12 years old, physical inactivity is strongly linked to depression.
Even anxiety, stress, and depression associated with menopause are less severe in those who exercise! So LET’S ALL GET OUT THERE AND EXERCISE!!!
Exercise Tip Of The Month

Women are often afraid to lift weights for fear they will look too “bulky”, but actually
that’s not what happens.
Women can and should do weight lifting exercises if they want to shed body fat and achieve a toned physique. Strength training 30 to 40 minutes twice a week for 4 months, could increase an average woman’s resting metabolism by 100 calories a day, meaning you’ll be burning calories even when you’re not exercising.
Trigger points in the triceps muscle.
The tricep muscle is named for its three heads long, medial, and lateral. The long head originates on the infraglenoid tubercle, the medial head on the posterior humerus, and the lateral head on the posterior humerus as well. They join together to insert on the Olecranon process of the ulna. The triceps function to extend the elbow. Strong extension under resistance can cause trigger points to form. Pain referred from triceps trigger points can be felt in the posterior shoulder and down the posterior forearm, as well as in in the olecranon process and the lateral epicondyle which can cause “tennis elbow” pain.
My knee hurts; I must have bad knees….

Due to bipedal locomotion (walking around on two legs), foot and ankle problems have the potential to affect EVERYTHING above the feet—even the knees!
When analyzing the way we walk (also known as our gait), we find when the heel strike takes place, the heel and foot motion causes “supination” or the rolling OUT of the ankle. As the unloaded leg begins to swing forwards, there is a quick transition to pronation where the heel and ankle roll inwards and the medial longitudinal arch (MLA) of the foot flattens and pronates NORMALLY!
During the transition from supination to pronation, the flattening of the MLA acts like a spring to propel us forwards followed by the “toe off”, the last phase, as we push off with our big toe and the cycle starts with the other leg. However, if you watch people walk from behind, you will see MANY ankles roll inwards too much. This is call “hyperpronation” and that is NOT NORMAL!
So at what point does this normal pronation become hyperpronation? The answer is NOT black and white, as there is no specific “cut-off” point but rather, a range of abnormal. Hence, we use the terms mild, moderate, and severe hyperpronation to describe the variance or the degrees of abnormality. Hyperpronation can lead to the development of bunions and foot/ankle instability that can cause and/or contribute to knee, hip, pelvis, and spinal problems—even neck and head complaints can result (the “domino effect”)!
One study looked at the incidence of hyperpronation in 50 subjects who had an anterior cruciate ligament (ACL) rupture vs. 50 without a history of knee / ACL injury. They found the ACL-injured subjects had greater pronation than the noninjured subjects suggesting that the presence of hyperpronation increases the risk of ACL injury.
Doctors of chiropractic are trained to evaluate and treat knee conditions of all kinds. Often this may include prescribing exercises or utilizing foot orthotics in an effort to restore the biomechanics of the foot, which can have positive effects not only on the knees but also further up the body.
