The quadratus lumborum muscle is a commonly overlooked source of low back pain and is often responsible for “pseudo disc syndrome”. This muscle originates on the inferior border of the 12th rib and lumbar transverse processes. It inserts on the iliac crest and iliolumbar ligament. The q.l.’s main actions are extension and lateral flexion of the spine. It also acts as a stabilizer of the lumbar spine. Trigger points in this muscle refer pain into the sacroiliac joint and the lower buttock. Pain can also spread anteriorly along the crest of the ilium into the lower abdomen and groin and to the greater trochanter. 
Fitness
Runner’s Knee Sucks.
Patellofemoral pain syndrome (PFPS) describes a painful irritation of the cartilage behind your kneecap. Although anyone may be affected, it is often the result of overuse of the knee in sports that require jumping or running so it is sometimes referred to as “Runner’s knee”. PFPS is the most common cause of knee pain in the general population, affecting an estimated 25% of adults.

One of the most common causes of PFPS is an imbalance between the muscles that help to guide your kneecap in its V-shaped groove at the end of your thigh bone. Repeatedly flexing and extending a misaligned kneecap leads to pain, swelling and eventually arthritis. Misalignment of the kneecap (patella) is often secondary to problems in the hip and foot, especially weakness of your gluteal muscles or flat feet.
PFPS produces a dull pain behind the kneecap that is aggravated by prolonged walking, running, squatting, jumping, stair climbing or arising from a seated position. The pain is often worse when walking downhill or down stairs. Longstanding misalignment can cause damage to the cartilage, which results in popping, grinding or giving way.
Conservative care, like the type provided in this office, is generally successful at relieving your symptoms. Initially, it is important for you to minimize activities that provoke your pain, especially running, jumping and activities that stress you into a “knock-kneed” position. Don’t allow your knees to cross in front of your toes when squatting. Some athletes may need to modify their activity to include swimming or bicycling instead of running.
Performing your home exercises consistently is one of the most important things that you can do to help realign the patella, relieve pain and prevent recurrence. The use of home ice or ice massage applied around your kneecap for 10-15 minutes, several times per day may be helpful.
What is Tarsal Tunnel Syndrome?
The tarsal tunnel is the space behind the bump on the inside of your ankle. The tibial nerve lives in this tunnel along with some tendons. Tarsal tunnel syndrome means that the tibial nerve is being irritated within the tunnel. This results in pain, numbness or tingling into your heel and the arch of your foot.
The tibial nerve may be irritated by compression (from trauma , arthritic spurs, or swelling of other tissues within the tunnel), or more commonly by constant stretch (from flat feet). Research has shown that tarsal tunnel pressure increases almost 30 fold in people with flat feet.
 Tarsal tunnel is slightly more common in women, and high heels are suspect. The condition often affects both feet. Conditions like diabetes and thyroid disorders may aggravate nerve problems like tarsal tunnel. Plantar fasciitis commonly accompanies tarsal tunnel syndrome.
Tarsal tunnel is slightly more common in women, and high heels are suspect. The condition often affects both feet. Conditions like diabetes and thyroid disorders may aggravate nerve problems like tarsal tunnel. Plantar fasciitis commonly accompanies tarsal tunnel syndrome.
The discomfort is often described as “burning”. Symptoms may increase with long periods of standing, running or exercise. Almost half of patients report increased symptoms at night.
Your doctor will make the diagnosis of tarsal tunnel syndrome based on your history and an exam. Your doctor may take an x-ray to rule out other problems like arthritic spurs or a stress fracture. In severe cases, more sophisticated nerve testing may be necessary.
The first goal of treatment is to allow you to return to pain-free activity as soon as possible. The second goal is to correct the mechanical problem that allowed this condition to begin with.
What is a knee sprain?
“Ligaments” are made up of many individual fibers running parallel to each other and bundled to form a strong fibrous band. These fibrous bands hold your bones together. Just like a rope, when a ligament is stretched too far, it begins to fray or tear. “Sprain” is the term used to describe this tearing of ligament fibers.


Sprains are graded by the amount of damage to the ligament fibers. A Grade I sprain means the ligament has been painfully stretched, but no fibers have been torn. A Grade II sprain means some, but not all of the ligamentous fibers, have been torn. A Grade III sprain means that all of the ligamentous fibers have been torn, and the ligament no longer has the ability to protect the joint. Knee sprains commonly involve one or more of your knee’s ligaments including: the medial collateral, lateral collateral, anterior cruciate, and posterior cruciate.
Most knee sprains begin as the result of a sudden stop, twist, or blow from the side or front. Some patients recall a “pop” or “snap” at the time of injury. Knee sprains cause pain and swelling within the joint. Your knee may be tender to touch, and some patients report a sensation of “giving way” or difficulty walking.
Most knee sprains can be successfully managed without surgery but will require some work on your part. Initially, a period of rest may be necessary in order to help you heal. Mild Grade I sprains may return to activity in a couple of days, while more severe injuries may take six weeks or longer to recover. You can help reduce swelling by elevating your knee and using an ACE wrap for compression. Applying ice or ice massage for 10 minutes each hour may help relieve swelling. Depending upon the severity of your sprain, you may need to wear a knee brace to help protect you from further injury. If walking is painful, crutches may be necessary.
I’ve got Shin Splints; what do I do?
Shin splints, also called “Medial Tibial Stress Syndrome,” (MTSS) is caused when the muscles of your lower leg pull too hard on your bone, causing local pain and inflammation. Over half of all leg pain in athletes is caused from shin splints. Up to 1/3 of runners and soldiers experience shin splints at some point in their lifetime.
MTSS is an overuse injury frequently seen in sports involving running, jumping, or frequent stopping & starting, i.e. field hockey, soccer and cross-country. Shin splints do not occur overnight but over a period of time, often show up during the first two or three weeks of training for a new season. Shin splints can occur when there are changes to your exercise regimen, such as an increase in activity, change in shoes or a change in the surface you play on. Some doctors refer to these training areas as “the terrible toos,” – too much, too hard, too long, too fast.

Symptoms of shin splints include tenderness or pain over the inside lower portion of your shin. The discomfort begins at the start of exercise and eases as you continue. Some patients report “bumps” when touching the inner portion of their leg bone. Be sure to tell your doctor if you experience weakness, numbness or cold feet during exercise or find a very small area of sensitivity.
Unfortunately, MTSS usually develops during a time when you are training heavily for a sport or an upcoming event. Continuing this activity will often lead to ongoing problems and decreased performance. Shin splints are now believed to be a forerunner to stress fracture, so adequate rest is critical. You may need to consider non-weight bearing cross training, such as using a stationary cycle or pool running.
When directed, your return to activity should start slowly, beginning with a 1/4 mile run and progressing by 1/4 mile each time you have no pain for two consecutive workouts. You should initially avoid running on hard or uneven surfaces and begin at a lower intensity and distance, increasing by no more than 10-15% per week- first increase distance, then pace, and avoid hard or unlevel surfaces, including hills.
Sports creams and home ice massage may provide some relief. Use ice after any activity. Patients who have flat feet are predisposed to developing shin splints and may need arch supports or orthotics. Avoid using heel cushions in your shoes, as they may increase the recurrence of this problem.
Trigger points in the serratus anterior
The serratus anterior muscle is located along the sides of the ribs. It originates on the outer surface of the upper 8-9ribs, and inserts on the medial border of the scapula. This muscle acts on the scapula in several different ways. First it rotates the scapula to turn the glenoid fossa upward. It also protracted and elevates the scapula. And lastly it helps to prevent wining. This muscle is often shortened from prolonged sitting and work on a computer. Active trigger points in this muscle refer pain locally around the trigger point with spillover down the inside of the arm. Pain can also radiate into the inferior angle of the scapula. 
Trigger points in the iliopsoas muscle
This muscle originates on the bodies and disks of T12-L5 and the inner ilium. It inserts on the lesser trochanter of the femur. The psoas flexes the hip when the spine is fixed. When the leg is fixed it extends the lumbar spine increasing lumbar lordosis. This Muscle is often chronically shortened due to inactivity and sitting posture. When trigger points are present they will refer pain primarily to the lower lumbar area and the sacrum as well as into the anterior thigh. Trigger points in the iliopsoas muscle can mimic appendicitis.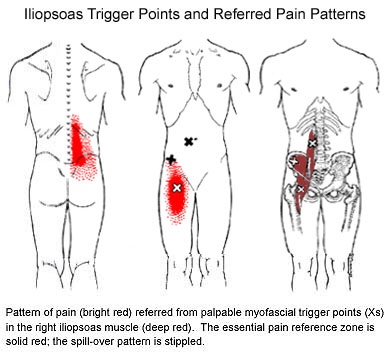
What is Fibromyalgia?
Fibromyalgia, although often misdiagnosed and misunderstood, is the second most common musculoskeletal disorder behind osteoarthritis. The condition affects nearly 12 million Americans and is ten times more common in women.
The diagnosis of fibromyalgia is made when a certain set of symptoms has been present for at least three months. The most common symptoms include wide-spread muscle and joint pain, achiness or soreness- especially in the neck, shoulders, back, and hips. Your muscles may constantly feel overworked and tired. Fibromyalgia patients often exhibit a set of predictable “tender points” spread throughout the body. Some patients have trouble sleeping and feel as though they are in a “brain fog” most of the day. This can lead to fatigue or mood changes, like anxiety and depression.

Stress is a known contributor to fibromyalgia, and patients should seek ways to de-stress, including yoga or meditation. Fibromyalgia patients should minimize their caffeine intake, as this is a known stimulant for nervousness, anxiety, and insomnia. Breathing exercises are sometimes helpful.
Although your sleep may be restless, you should try to establish a bedtime routine that gives your body the best chance for recovery. Try to avoid late night electronics, like the television or computer. Keep your bedroom dark, quiet, cool, and distraction-free. Be sure to take time for yourself each day for relaxation or to do something you enjoy. Combat “brain fog” by carrying a notebook or a phone to make notes for important things. Some patients report decreased muscle tightness by applying moist heat or a taking warm bath. The American Pain Society recommends conservative treatment, including chiropractic, along with moderate aerobic exercise.
Trigger points in the piriformis muscle
The piriformis muscle is a small muscle deep to glute max and lies over top of the sciatic nerve. It originates on the anterior sacrum, and inserts on the greater trochanter of the femur. It’s main action is to laterally rotate the femur. When trigger points developed in this muscle they will refer pain into the sacro-iliac region, across the posterior hip and down the leg. This muscle can also be a cause of sciatic nerve irritation if it gets tight, causing “sciatica” symptoms. 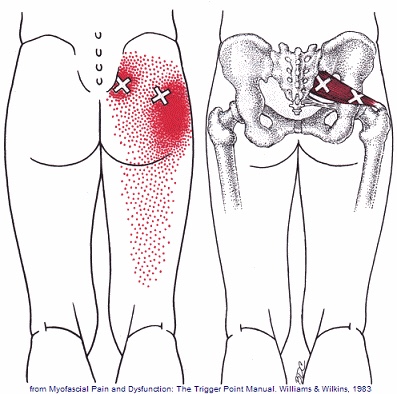
Scapular Dyskinesis (Yes, its a thing).
Your shoulder is formed by three bones; the scapula (shoulder blade), the clavicle (collar bone), and the humerus (long arm bone.) These bones come together to form a shallow ball & socket that relies upon the surrounding muscles for support. All of your shoulder muscles must work in a coordinated fashion to have a healthy and stable joint. Disruption of the normal rhythm of your shoulder blade creates abnormal strain on your shoulder and rotator cuff called “Scapular dyskinesis”. This dysfunction crowds the area of your shoulder where your rotator cuff tendons live and may create a painful pinching of your tendons or bursa each time you raise your arm. Many shoulder problems, including sprains/strains, tendinitis, bursitis, or rotator cuff irritation, result from this often overlooked culprit.

Scapular dyskinesis most commonly originates from weakness or imbalance of the muscles that control your shoulder blade. Sometimes the problem is caused by other shoulder conditions like prior fractures, arthritis, or instability. Irritation of the nerves that control the shoulder muscles is the culprit in about 5% of cases.
Although scapular dyskinesis can cause a variety of shoulder problems, it may initially go unnoticed. Up to 75% of healthy college athletes show some form of abnormal shoulder blade movement. If the condition is left untreated, you may begin to notice pain near the top of your shoulder. Sometimes the discomfort can radiate toward your neck or into your arm. Patients will often complain of a tender spot on the front of their shoulder. Long-standing altered mechanics can lead to bigger problems, including rotator cuff injury, shoulder instability, and arthritis.
The good news is that we have recognized the underlying cause of your shoulder problems and have treatments to correct it. You will need to perform your exercises consistently. You should also be conscious of your posture and try to avoid sitting or standing in “slouched” positions, as this is known to aggravate your problem.
