The gluteus medius muscle plays an important role in hip and pelvic stability. It originates on the gluteal surface of the ilium, deep to the gluteus Maximus. It inserts on the greater trochanter of the femur. It’s main actions are to abduct the hip and to assist in internal rotation of the hip. It also maintains pelvic stability during walking and running. Trigger points in this muscle will refer pain into the sacrum, the iliac crest, and down the lateral hip and into the thigh. This muscle is often a cause of lower pack pain.
Canada
The High Ankle Sprain (Don’t Let This Happen To You. These SUCK.)
Your lower leg bones (tibia and fibula) are held together at the ankle by a group of soft tissues and ligaments called the “syndesmosis”. This connection prevents excessive spreading of these bones during normal activity, but injuries can cause these ligaments to be stretched or torn. This problem is called a “syndesmotic ankle sprain” or “high ankle sprain”. High ankle sprains often occur during contact sports (like football, hockey, and soccer) when your foot is planted while the rest of your body shifts forward and turns inward. High ankle sprains are much less common than other types of ankle sprains.

The pain of a high ankle sprain starts just above your ankle and runs up your shin. Interestingly, the “length” of pain correlates very closely to your severity of injury. Standing and walking is usually uncomfortable and sometimes unbearable. Bringing your toes toward your shin or rotating your foot outward will likely increase your pain. Significant bruising or swelling is possible. Be sure to tell your doctor if you notice numbness, tingling, or coldness in your foot.
Ankles that have suffered a complete separation usually require surgery, since they will have lost the ability to push off, propel, and cut. Most other stable sprains will respond to conservative care, like the type provided in this office. It is important to recognize that high ankle sprains heal more slowly than other types of ankle sprains. The average recovery time for a syndesmotic sprain is between two and seven weeks but some injuries may require up to four months away from your sport. You may need to wear a boot or avoid weight bearing for a period of time. Ice may help to limit swelling initially, and the home exercises described below are an important part of your recovery.
Achilles Tendonitis: The Details
Your Achilles tendon is the strong fibrous band of tissue that connects your calf muscles to your heel. The tendon is named after “Achilles” who was a powerful, yet vulnerable warrior in Greek mythology. Likewise, our Achilles tendon, being the largest and strongest tendon in the body, is susceptible to injury from the high demands placed on it. (Running can generate forces over 12 times your bo

dy weight on the Achilles tendon.)
The tendon may be strained or even ruptured from excessive stretch or forceful contraction of the calf muscles. More commonly, the tendon is repeatedly overloaded and suffers tiny “micro tears.” Damage usually occurs either directly behind the heel, or near the weakest area of the tendon- one to two inches above the heel.
Achilles tendon injuries affect between 250,000 and 1 million people per year. Most are middle-aged males, between the age of 30 and 50. Interestingly, Achilles tendon injuries occur more frequently on the left side. If you have suffered a prior Achilles tendon injury, you are at greater risk of injuring the opposite side. Two-thirds of all Achilles tendon injuries involve athletes. Runners are up to 10 times more likely to suffer Achilles tendon problems. You may at increased risk if the arch of your foot is too high or too flat.
Symptoms may begin abruptly following a strain but more commonly develop slowly from repeated irritation. Morning pain and stiffness are common. Your symptoms will likely increase with activity, especially walking or running. You may notice pain when you rise up on your toes. Walking down stairs stretches the tendon and usually increases symptoms. Some patients notice that the irritated area becomes firmly swollen. Ongoing irritation to the spot on your heel where the tendon inserts can cause a painfully elevated “pump bump.”
Research has shown that conservative care, like the type provided in this office, can produce “excellent results” in over 85% of patients. Initially, you may need to limit or stop activities that cause pain. Runners may need to switch to swimming or cycling for a short period of time. Be sure to introduce new activities slowly and avoid increasing your activity by more than 10% per week. Runners should begin on a smooth, shock-absorbent surface and start at a low intensity – first increasing distance, then pace. Avoid training on hard or unlevel surfaces like hills. Make sure you warm up properly and avoid over training. Avoid wearing high heels or shoes with an excessively rigid heel tab. One of the most important and effective treatments for Achilles tendinopathy is performing “heel drop exercises” as outlined below.
Eccentric Achilles Strengthening
Begin standing up on your toes with the affected foot on the edge of a step. Do not place weight on your good leg, but you may use it for stability. Slowly lower your affected heel, at a count of 4 seconds, until you reach a fully stretched position and can drop no further. Use your good leg to return to your toes. Repeat 3 sets of 15 repetitions with your knee straight and 3 more sets of 15 repetitions with your knee slightly bent, twice daily or as directed. Moderate pain during this exercise is acceptable but if pain is excessive, you should assist downward motion with the non-injured leg.
Here is a brief description of the treatments we may use to help manage your problem.
 Joint Manipulation
Your chiropractor has found joints in your body that are not moving freely. This can cause tightness and discomfort and can accelerate unwanted degeneration i.e. arthritis. Your chiropractor will apply a gentle force with their hands, or with hand held instruments, in order to restore motion to any “restricted” joints. Sometimes a specialized table will be used to assist with these safe and effective “adjustments”. Joint manipulation improves flexibility, relieves pain and helps maintain healthy joints.
 Therapy Modalities
We may apply electrotherapy modalities that produce light electrical pulses transmitted through electrodes placed over your specific sites of concern. These comfortable modalities work to decrease your pain, limit inflammation and ease muscle spasm. Hot or cold packs are often used in conjunction, to enhance the effect of these modalities. Another available option is therapeutic ultrasound. Ultrasound pushes sound vibrations into tissues. When these vibrations reach your deep tissues, heat develops and unwanted waste products are dispersed.
 Myofascial Release
Overworked muscles often become tight and develop knots or “trigger points”. Chronic tightness produces inflammation and swelling that ultimately leads to the formation of “adhesions” between tissues. Your chiropractor will apply pressure with their hands, or with specialized tools, in order to release muscle tightness and soft-tissue adhesions. This will help to improve your circulation, relieve pain and restore flexibility.
 Therapeutic Exercise
Muscle tightness or weakness causes discomfort and alters normal joint function, leading to additional problems. Your chiropractor will target tight or weak muscles with specific therapeutic stretching and strengthening to help increase tissue flexibility, build strength, and ease pain. Healthy, strong, and flexible muscles may help prevent re-injury.
 Elastic Therapeutic Tape
Your chiropractor may apply a special elastic therapeutic tape in order to support injured areas or encourage better movement. This tape is thought to decrease pain and swelling, improve circulation and limit muscle soreness.
 Foot Evaluation
Fallen arches and faulty foot mechanics are common problems that can perpetuate your condition. Our office will carefully evaluate your feet and consider the need for a change in shoe style, arch supports or even custom orthotics.
 Ankle Brace
Our office may recommend using a support brace to protect your ankle from further injury. Your doctor will discuss the specific type of brace and provide instructions for use.
|
||
|
After this initial course of treatment we will reassess your progress. We will determine the need for any additional care after your reassessment.
|
||
Trigger points in the gluteus Maximus
The gluteus Maximus is the buttock muscle. It originates on the gluteal surface of the ilium, lumbar fascia, sacrum and sacrotuberous ligament. It inserts on the gluteal tuberosity of the femur and the iliotibial tract. Extension and lateral rotation of the hip are it’s main actions. This muscle is heavily involved in activities like ice skating and is a common area to develops trigger points. When trigger points do develop they can refer pain in a crescent pattern from the gluteal fold to the sacrum. Trigger points can also refer pain deep into the buttock itself making it feel like other deeper muscles are involved. These symptoms can sometimes be mistaken for s.i. Joint problems. 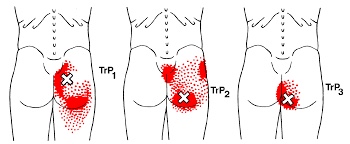
Trigger points in the supraspinatus
The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.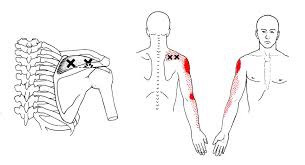
Trigger points in the infraspinatus
The infraspinatus muscle is one of the muscles that makes up the rotator cuff. It originates on the infraspinous fossa of the scapula, and inserts on the middle facet of the greater tubercle of the humerus. It functions to externally rotate the humerus and to stabilize the head of the humerus in the glenoid cavity during upward movement of the arm. Trigger points in this muscle refer pain deep into the anterior shoulder joint and down the anterior arm. Trigger points near the lower medial border refer pain into the rhomboids. This muscle is often injured during throwing motions.
Is there an actual cure all?

No; but exercise seems to be as close as we will ever get!
Some of you may have heard about how a modified form of boxing is helping patients with Parkinson’s disease (PD). If you haven’t, it’s been observed that people with Parkinson’s disease (PD) who engage in this boxing-like exercise routine can enhance their quality of life and even build impressive gains in posture, strength, flexibility, and speed. Proponents of the program report that regardless the degree of severity of PD, participants have a happier, healthier, and higher quality of life.
But must it be boxing? Maybe not. A report presented at the International Congress of Parkinson’s Disease and Movement Disorders in San Diego in June 2015 found that patients with Parkinson’s disease who began regular exercise early into the PD process had a much slower decline in their quality of life when compared with those who started exercising later. The researchers found just 2.5 hours per week of exercise is needed to improve quality of life scores. According to the report, it didn’t matter what exercise the participants did — simply getting up and moving for a total of 2.5 hours/week was reportedly enough (that’s only 20-25 minutes / day)!
Looking beyond Parkinson’s, other chronic conditions also benefit from adding exercise into a person’s lifestyle. Studies show that regular exercise as simple as walking helps reduce one’s risk for memory loss, and it slows down functional decline in the elderly. Incorporating aerobic exercise into one’s lifestyle can also improve reaction time in people at ALL AGES. Exercise has also been shown to improve both physical and emotional well-being in those afflicted with Alzheimer’s disease with as little as 60 minutes/week of moderate exercise! Patients with multiple sclerosis (MS) have also reported less stiffness and less muscle wasting when using exercise machines, aquatic exercise, and/or walking.
Research has shown just 30 minutes of brisk exercise three times a week can help reduce depressive symptoms in patients with mild-to-moderate depression. In a study involving teenagers, those who engaged in sports reported a greater level of well-being than their sedentary peers, and the more vigorous the exercise, the better their emotion health! In kids 8-12 years old, physical inactivity is strongly linked to depression.
Even anxiety, stress, and depression associated with menopause are less severe in those who exercise! So LET’S ALL GET OUT THERE AND EXERCISE!!!
Trigger points in the triceps muscle.
The tricep muscle is named for its three heads long, medial, and lateral. The long head originates on the infraglenoid tubercle, the medial head on the posterior humerus, and the lateral head on the posterior humerus as well. They join together to insert on the Olecranon process of the ulna. The triceps function to extend the elbow. Strong extension under resistance can cause trigger points to form. Pain referred from triceps trigger points can be felt in the posterior shoulder and down the posterior forearm, as well as in in the olecranon process and the lateral epicondyle which can cause “tennis elbow” pain.
Chronic Lumbar Disc Pain
Your low back consists of 5 individual vertebrae stacked on top of each other. Flexible cushions called “discs” live between each set of vertebrae. A disc is made up of two basic components. The inner disc, called the “nucleus”, is like a ball of jelly about the size of a marble. This jelly is held in place by the outer part of the disc called the “annulus”, which is a tough ligament that wraps around the inner nucleus much like a ribbon wrapping around your finger.

Your low back relies on discs and other ligaments for support. “Discogenic Low Back Pain” develops when these tissues are placed under excessive stress, much like a rope that frays when it is stretched beyond its normal capacity. Most commonly, disc pain is not the result of any single event, but rather from repeated overloading. Your lumbar discs generally manage small isolated stressors quite well, but repetitive challenges lead to injury in much the same way that constantly bending a piece of copper wire will cause it to break. Examples of these stressors include: bad postures, sedentary lifestyles, poor fitting workstations, repetitive movements, improper lifting, or being overweight.
Approximately one third of adults will experience pain from a lumbar disc at some point in their lifetime. The condition is more common in men. Most lumbar disc problems occur at one of the two lowest discs- L5 or L4. Smokers and people who are generally inactive have a higher risk of lumbar disc problems. Certain occupations may place you at a greater risk, especially if you spend extended periods of time sitting or driving. People who are tall or overweight have increased risk of disc problems.
Symptoms from disc pain may begin abruptly but more commonly develop gradually. Symptoms may range from dull discomfort to surprisingly debilitating pain that becomes sharper when you move. Rest may relieve your symptoms but often leads to stiffness. The pain is generally centered in your lower back but can spread towards your hips or thighs. Be sure to tell your doctor if your pain extends beyond your knee, or if you have weakness in your lower extremities or a fever.
Repeated injuries cause your normal healthy elastic tissue to be replaced with less elastic “scar tissue.” Over time, discs may dehydrate and thin. This process can lead to ongoing pain and even arthritis. Patients who elect to forego treatment and “just deal with it” develop chronic low back pain more than 60% of the time. Seeking early and appropriate treatment like the type provided in our office is critical.
Depending on the severity of your injury, you may need to limit your activity for a while, especially bending, twisting, and lifting, or movements that cause pain. Bed rest is not in your best interest. You should remain active and return to normal activities as your symptoms allow. Light aerobic exercise (i.e. walking, swimming, etc) has been shown to help back pain sufferers. The short-term use of a lumbar support belt may be helpful. Sitting makes your back temporarily more vulnerable to sprains and strains from sudden or unexpected movements. Be sure to take “micro breaks” from workstations for 10 seconds every 20 minutes.
Pathophysiology of trigger points.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.
