In 2010, Dr. Gert Bronfort published a pinnacle report that reviewed studies published up to 2009 and identified 26 categories of conditions for which there is evidence that manual therapies (including spinal manipulation, mobilization, and massage) are beneficial. These 26 categories included thirteen musculoskeletal (MSK) conditions (like low back and neck pain), four types of chronic headache, and nine non-MSK conditions (like infantile colic).
In 2014, the 2010 study was “updated” by Dr. Christine Clar and five colleagues from the Warwick Medical School in the United Kingdom using the same methodologies. They concentrated on the conditions that resulted in a “negative” or an “inconclusive” result in 2010 and either confirmed, updated, or added a new category based on the results of newer research.
After reviewing 25,539 studies, other conditions such as shoulder rotator cuff disorder, cervicogenic headache, and other types of headaches were added to the list. They also added a large number of non-MSK conditions they had not previously considered, of which most were rated ‘inconclusive.’
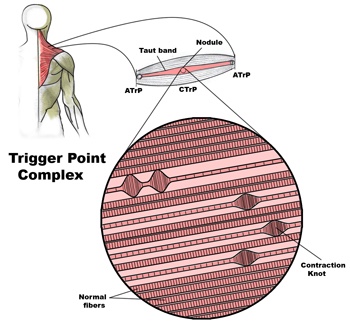
The 2014 study pointed out the continued need for more high-quality research on many conditions, but it shed light on a significant number of conditions not previously reported in the 2010 study such as TMD (jaw pain), myofascial pain syndrome, active upper trapezius trigger points and neck pain, carpal tunnel syndrome, tennis elbow, shoulder disorders, nerve and muscle pain in the shoulder, plantar fasciitis, arthritis with and without angulation of the great toe (big toe), and many more!
The non-MSK conditions that Dr. Clar and her team found that are in need of further high-quality studies include: asthma, cervicogenic dizziness, hypertension, infantile colic, enuresis, pneumonia/respiratory disorders, dysmenorrhoea, and PMS. “NEW” categories include: ADHD/learning disorders, cancer care, cerebral palsy, chronic fatigue, chronic pelvic pain, cystic fibrosis, gastrointestinal, menopause, Parkinson’s disease, pregnancy and neonatal and post-natal care, rehabilitation, and peripheral arterial disease.
Obviously, these two studies have taken the quest of determining the current “science” behind many of the claims that doctors of chiropractic have made for many conditions HEAD ON. This is a VERY important step in the right direction so we as healthcare professionals can tell our patients which conditions are likely or not likely to respond to this form of care based on research!