
Happy New Year 2018!!!!


Fibromyalgia (FM) and its cause remains a mystery, but most studies suggest that FM is NOT the result of a single event but rather a combination of many physical, chemical, and emotional stressors.
The question of the month regarding the BEST FM diet is intriguing since one might assume that the many causes should mean that there isn’t one dietary solution. But is that true? Could there be a “best diet” to help ease the symptoms from such a multi-faceted disorder?
Certainly, healthy eating is VERY important for ALL of us regardless of our current ailment(s). Obesity is rampant largely due to the fact that 60% of the calories consumed by the “typical” American center around eating highly inflaming food that include those rich in Sugar, Omega-6 oil, Flour, and Trans fats (“SOFT” foods, if you will!). Obesity has been cited as “an epidemic” largely due to kids and adults becoming too sedentary (watching TV, playing on electronic devices, etc.) and eating poorly.
Perhaps the BEST way to manage the pain associated with FM and to maintain a healthy BMI (Body Mass Index, or ratio between height and weight) is to substitute ANTI-INFLAMING foods for those that inflame (or SOFT foods).
You can simplify your diet by substituting OUT “fast foods” for fruits, vegetables, and lean meats. So there you have it. It’s that simple. The problem is making up your mind to change and then actually doing it. Once these two things take place, most everyone can easily “recalibrate” their caloric intake and easily adapt.
Not only have studies shown that chronic illnesses like heart disease, stroke, and diabetes significantly benefit by following this simple dietary shift, but so does pain arising from the musculoskeletal system! This is because the human body is made up largely of chemicals, and chemical shifts are constantly taking place when it moves. If you reach for an anti-inflammatory drug like ibuprofen or naproxen and it helps, it’s because you ARE inflamed and the drug reduces the pain associated with that inflammation. This is an indication that an anti-inflammatory diet WILL HELP as well (but without the negative side effects)!
The list of chronic conditions that result in muscle pain not only includes FM but also obesity, metabolic syndrome, and type II diabetes. Conditions like tension-type and migraine headaches, neck and back pain, disk herniation, and tendonopathies and MANY more ALL respond WELL to making this SIMPLE change in the diet. For more information on how to “DEFLAME,” visit http://www.deflame.com! It could be a potential “lifesaver!”
Dizziness, neck pain, and headaches are very common symptoms that may or may not occur at the same time. Though this interrelationship exists, this month’s article will focus primarily on dizziness, particularly related to dizziness that occurs after standing.
First, it is important to point out that it is VERY common to be light headed or dizzy when standing up too fast, which is typically referred to as orthostatic hypotension (OH). OH is frequently referred to as a benign symptom, but new information may challenge this thought.
Let’s review what happens. When we are lying down, our heart does not have to work as hard as when we are upright; therefore, our blood pressure (BP) is usually lower while we lay in bed. When standing up, blood initially pools in the legs until an increase in blood pressure brings oxygen to the brain. This either resolves or prevents dizziness.
Orthostatic hypotension is defined as a blood pressure drop of >20 mm Hg systolic (the upper number—heart at FULL contraction), 10 mm Hg diastolic (lower number—heart at FULL rest), or both. This typically occurs within seconds to a few minutes after rising to a standing position.
There are two types of OH—delayed OH (DOH) where the onset of symptoms are not immediate but occur within three minutes of standing and “full” OH, which is more serious and occurs immediately upon rising. According to a 2016 study published in the prestigious journal Neurology, researchers reviewed the medical records of 165 people who had undergone autonomic nervous system testing for dizziness. The subjects averaged 59 years of age, and 48 were diagnosed with DOH, 42 with full OH, and 75 subjects didn’t have either condition.
During a ten-year follow-up, 54% of the DOH group progressed to OH, of which 31% developed a degenerative brain condition such as Parkinson’s disease or dementia. Those with initial DOH who also had diabetes were more likely to develop full OH vs. those without diabetes.
The early death rate in this 165 patient group was 29% for those with DOH, 64% with full OH, vs. 9% for those with neither diagnosed condition. The authors point out that those initially diagnosed with DOH who did NOT progress into full OH were given treatment that may have improved their blood pressure.
The authors state that a premature death might be avoided by having DOH and OH diagnosed and properly managed as early as possible. They point out that a prospective study is needed since this study only looked back at medical records of subjects who had nervous system testing performed at a specialized center, and therefore, these findings may not apply to the general population.
The value of this study is that this is the FIRST time a study described OH (or DOH) as a potentially serious condition with recommendations NOT to take OH/DOH lightly or view it as a benign condition. Since doctors see this a lot, a closer evaluation of the patient is in order.
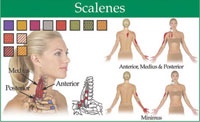
The scalene muscles are located in the neck and originate on c3-c6 and insert on the first and second rib. These muscles act to laterally flex the neck, and assist in respiration by helping to elevate the ribs. Trigger points can form in this muscle from acute injuries such as whiplash, or from chronic injury such as poor posture or shallow nervous breathing. Trigger points in these muscles can refer pain in two finger like projections into the chest. Other common patterns are into the shoulder, scapula and down the lateral arm, and into the thumb and index finger. The scalene muscle can impinge on the brachial plexus, causing nerve pain or numbness down the arm. This is called thoracic outlet syndrome.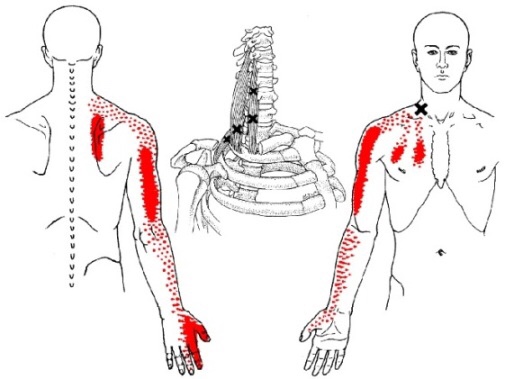
Carpal tunnel syndrome (CTS) can be an extremely painful and activity-limiting condition. It affects many people of all ages and genders, though women are affected more often than men. But how do you know if what you are suffering from is truly CTS or if it’s another condition that’s producing the symptoms in your hand or wrist?
Carpal tunnel syndrome occurs when the median nerve is compressed as it passes through the wrist. However, the median nerve travels out of the neck, through the shoulder, elbow, and forearm before it passes through the wrist and into the hand. Pinching of the median nerve ANYWHERE along its course can give rise to the signs and symptoms of CTS including numbness, tingling, and/or pain into the hand and index, third, and thumb-side half of the fourth digits, and sometimes the thumb. If the pinch is significant enough, weakness can also occur. Sometimes the median nerve can become compressed at both the wrist and other body sites as it travels from the spinal cord to your hand, that’s why it’s important for a doctor to check for impingements along the entire course of the nerve.
But compression of the median nerve isn’t the only thing that can produce symptoms in the hand. Here are a couple of the more common conditions that are often confused with CTS:
1) Ulnar neuropathy: This is pinching of the ulnar nerve (at the neck, shoulder, elbow, or wrist) but this gives rise to a similar numbness/tingling BUT into the pinky-side of the fourth and the fifth fingers (not the thumb-side of the hand). The most common pinch location is either at the neck or the inner elbow, the latter of which is called “cubital tunnel syndrome” or CuTS.
2) Tendonitis: There are a total of nine tendons that pass through the carpal tunnel that help us grip or make a fist. Similarly, there are five main tendons on the back side of the hand that allow us to open our hands and spread our fingers. ANY of these tendons can get strained or torn, which results in swelling and pain as well as limited function BUT there is usually NO NUMBNESS/TINGLING!
3) DeQuervain’s disease: This is really a tendonitis of an extensor tendon of the thumb and its synovial sheath that lubricates it resulting in a “tenosynovitis.” This creates pain with thumb movements, especially if you grasp your thumb in the palm of your hand and then bend your wrist sideways towards the pinky-side of the hand.
Chiropractors are well-trained to diagnose and treat patients with CTS. And if you don’t have CTS but another condition listed above, they can offer treatment (or a referral, if necessary) to help resolve it so you can return to your normal activities as soon as possible.

Begin in a push-up position with your knees resting on an exercise ball. Maintain a neutral spine, and do not allow your back to arch down towards the floor. Roll the ball from your thighs to your ankles by bending your knees and bringing them towards your chest. Slowly return to the start position. Perform three sets of 10 repetitions daily or as directed.




