Evidence-based chiropractors must routinely answer two questions:
- Does this patient have inflamed tissue or degenerated tissue?
- Has this injury resulted in a compensatory movement pattern?
Chiropractors treat the cause of dysfunction and not the just the pain—right? This becomes more challenging when patients present with an assortment of orthopedic diagnoses. Let’s be honest, we see the worst of the worst on a daily basis, and we are often the last option.
Identifying IF inflammation is a source of pain may be one of the biggest differentiators in your initial exam.
Chiropractors see patients in pain resulting from acute injuries. Newly injured tissue often contains an inflammatory component for healing. However, emerging clinical research tells us that reoccurring painful conditions often lack an inflammatory component. Effective treatment of pain is dependent on a clear understanding of whether inflammation is present or not.
Learn how to identify chemical vs. mechanical pain
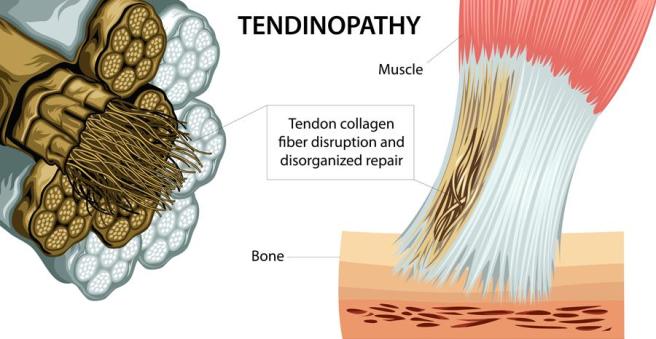
Many chronic tendon problems are not the result of ongoing inflammation, rather failed inflammation. Chronic failed inflammation results in tissue degeneration that diminishes long-term tissue capacity, size, and function. Tendons, when degenerated, exhibit lower stiffness. A failed healing response results in proliferation of tissue with decreased load transfer and elastic capability. We sometimes refer to this as scar tissue. This deficit must be accounted for during locomotion. Diminished tendon load transfer will lead to widespread biomechanical dysfunction. The patient must be willing to change their movement pattern or habits to stop this process.
Chronic problems often lead to widespread biomechanical dysfunction.
We have all seen the patient with chronic, but intermittent, plantar fasciitis who develops subsequent knee, hip, or back pain. Human movement is coordinated by a hierarchal system. The CNS initiates, controls and executes movement patterns. The human body knows movements—not muscles. If one tissue in the loop loses its integrity the patient may develop a new movement pattern. This new movement pattern may not be efficient to all the tissue components and result in new injuries. Our tissue only has a certain capacity. Muscles and tendons will strain, ligaments will sprain, and bones will break at different rates and/or amounts of load. Rehab should focus on optimal movement patterns instead of strengthening isolated muscles.
Let’s examine a patient with Achilles tendinosis?
Patients with Achilles pain will often favor the outside of their foot. Pain will result in an adaptive behavior altering the activity of agonist, synergist and antagonist muscles. A recent study in the Journal of Physiology highlighted this compensatory behavior:
“This was seen during single-legged hopping, where the contribution from the triceps surae muscle to the plantar flexors was decreased and the co-contraction from the tibialis anterior muscle was also decreased on the involved side in individuals with Achilles tendinosis. This may be attributed to the protective mechanism shielding the already injured tendon from further injury or even rupture.” (1)
If the agonist and antagonists have decreased activity, then how do these patients transfer load while walking?
“The EMG activity of the synergist muscle, the peroneal longus muscle in the present study, increased to compensate for the mechanical deficit resulting from the compliant Achilles tendon and to achieve the task goal.”
These patients have now condemned their gait cycle to walk on a supinated foot that transfers compensatory repercussions to the knee and hip. The increased load on the peroneal muscles may also result in injury in time. This is not an isolated problem, rather the typical continuum of an “…itis” to an “…opathy” over time. These are not isolated lesions; rather the start of widespread biomechanical dysfunction that may result in any number of orthopedic diagnosis. The authors conclude:
“Pain is a signal of tissue damage, although damaged tissues are not always painful.”
Excellent chiropractic clinical outcomes require that providers look upstream and downstream for biomechanical co-conspirators. ChiroUp helps your patients recognize how specific orthopedic conditions change movement patterns. Preselected exercise protocols incorporate ideal movement patterns during the rehab process. In the case of tendinopathy, ChiroUp protocols incorporate eccentric exercise to facilitate and strengthen the damaged tissue and prevent recurrence of pain.
Reference
- Chang Y-J, Kulig K. The neuromechanical adaptations to Achilles tendinosis. The Journal of Physiology. 2015;593(Pt 15):3373-3387. doi:10.1113/JP270220.