What is stopping you?

Fibromyalgia (FM) is a common condition that affects about five million Americans, often between ages 20 and 45 years old. FM is very difficult to diagnose primarily because there is no definitive test like there is for heart, liver, or kidney disease. Equally challenging is the ability to effectively treat FM as there are frequently other conditions that co-exist with FM that require special treatment considerations. Typically, each FM case is unique with a different group of symptoms and therefore, each person requires individualized care.
Fibromyalgia symptoms can include generalized pain throughout the body that can vary from mild to severely disabling, extreme fatigue, nausea/flu-like symptoms, brain “fog” (“fibro-fog”), depression and/or anxiety, sleeping problems and feeling un-refreshed in the mornings, headaches, irritable bowel syndrome, morning stiffness, painful menstrual cramps, numbness or tingling (arms/hands, legs/feet), tender points, urinary pain or burning, and more!
So, let’s talk about ways to improve your FM-related symptoms through dietary approaches. When the FM symptom group includes gut trouble (bad/painful gas, bloating, and/or constipation), it’s not uncommon to have an imbalance between the “good” vs. the “bad” bacteria, yeast, and problems with digestion or absorption. Think of management as a “Four Step” process for the digestive system:
1. REMOVE SENSITIVITIES: Consider food allergy testing to determine any foods the FM patient has a sensitivity for. Frequently, removing gluten, dairy, eggs, bananas, potatoes, corn, and red meat can benefit the FM patient. The use of anti-fungal and / or anti-bacterial botanicals (as opposed to drug approaches such as antibiotics) can be highly effective. A low allergy-potential diet consisting of fish, poultry, certain vegetables, legumes, fruits, rice, and olive and coconut oil is usually a good choice.
2. IMPROVE DIGESTIVE FUNCTION: The presence of bloating and gas is usually indicative of poor digestion, and the use of a digestive enzyme with every meal can be highly effective!
3. RESTORE THE “GOOD” BACTERIA: Probiotics (with at least 20-30 billion live organisms) at each meal are often necessary to improve the “good” gut bacteria population, which will likely also improve immune function.
4. REPAIR THE GUT: If the gut wall is damaged, nutrients like l-glutamine, fish oils, and n-acetyl-d-glucosamine may help repair it.
This process will take several months, and some of these approaches may have to be continued over the long term. Doctors of chiropractic are trained in nutritional counseling and can help you in this process. As an added benefit, many FM sufferers find the inclusion of chiropractic adjustments to be both symptomatically relieving and energy producing.
If you, a friend or family member requires care for Fibromyalgia, we sincerely appreciate the trust and confidence shown by choosing our services!

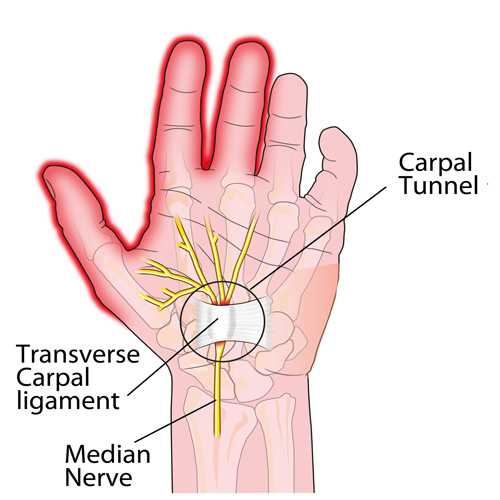
Here it is: carpal tunnel syndrome (CTS) in a nutshell!
Define what makes you your best self. Define what makes you happy, healthy and well and stop at nothing to get there.

Some things to consider if you’re suffering from back pain.
Reasons you’re probably suffering from back pain (besides sitting all day)
Whiplash Associated Disorders (WAD) is the appropriate terminology to use when addressing the myriad of symptoms that can occur as a result of a motor vehicle collision (MVC). In a recent publication in The Physician and Sports Medicine (Volume 43, Issue 3, 2015; 7/3/15 online:1-11), the article “The role of the cervical spine in post-concussive syndrome” takes a look at the neck when it’s injured in a car accident and how this relates to concussion.
It’s estimated about 3.8 million concussion injuries, also referred to as “mild traumatic brain injury” (mTBI), occur each year in the United States. Ironically, it’s one of the least understood injuries in the sports medicine and neuroscience communities. The GOOD NEWS is that concussion symptoms resolve within 7-10 days in the majority of cases; unfortunately, this isn’t the case with 10-15% of patients. Symptoms can last weeks, months, or even years in this group for which the term “post-concussive syndrome” (PCS) is used (defined as three or more symptoms lasting for four weeks as defined by the ICD-10) or three months following a minor head injury (as defined by the Diagnostic and Statistical Manual of Mental Disorders).
There have been significant advances in understanding what takes place in the acute phase of mTBI, but unfortunately, there is no clear physiological explanation for the chronic phase. Studies show the range of force to the head needed to cause concussion is between 60-160g (“g” = gravity) with 96.1g representing the highest predictive value in a football injury, whereas as little as 4.5g of neck acceleration can cause mild strain injury to the neck. In spite of this difference, the signs and symptoms reported by those injured in low-speed MVCs vs. football collisions are strikingly similar!
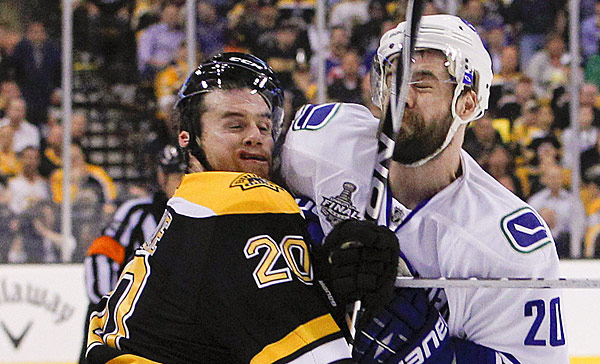
Research shows if an individual sustains an injury where the head is accelerated between 60-160g, it is HIGHLY likely that the tissues of the cervical spine (neck) have also reached their injury threshold of 4.5g. In a study that looked at hockey players, those who sustained a concussion also had WAD / neck injuries indicating that these injuries occur concurrently. Injuries to the neck in WAD include the same symptoms that occur in concussion including headache, dizziness/balance loss, nausea, visual and auditory problems, and cognitive dysfunction, just to name a few.
The paper concludes with five cases of PCS that responded well to a combination of active exercise/rehabilitation AND passive manual therapy (cervical spine manipulation). The favourable outcome supports the concept that the neck injury portion of WAD is a very important aspect to consider when treating patients with PCS!
This “link” between neck injury and concussion explains why chiropractic care is essential in the treatment of the concussion patient! This is especially true when the symptoms of concussion persist longer than one month!
We realize you have a choice in whom you consider for your health care provision and we sincerely appreciate your trust in choosing our service for those needs. If you, a friend, or family member requires care for Whiplash, we would be honoured to render our services.