Your radial nerve begins in your neck and travels past your elbow en route to its final destination in your hand. Just beyond your elbow, this nerve passes through a 2-inch area on the back of your forearm called the “Radial tunnel”. “Radial tunnel syndrome” means that your radial nerve has been compressed or irritated within this space-leading to forearm pain or hand weakness.

Radial tunnel syndrome is thought to result from muscular overuse, especially prolonged or excessive wrist extension or rotation. The most common cause of compression comes from excessive tightness in a muscle called the “Supinator”. Workers whose jobs require heavy or repetitive wrist movements are at an increased risk for this disorder. Occasionally, the radial nerve can become irritated from direct compression by a tight band or brace. The condition may be more common in those who have diabetes or thyroid problems.
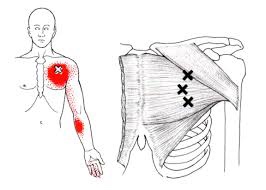
Symptoms from irritation of the radial nerve depend upon which specific nerve fibers are irritated. The most common symptoms include pain, numbness, tingling or decreased sensitivity along the top of your forearm radiating toward your hand and thumb. The symptoms often mimic those of “tennis elbow.” When the nerve fibers that control muscle function become compressed, you may experience weakness when trying to extend your fingers, hand or wrist. Seventy percent of radial tunnel patients also have problems in their neck or upper back.
Conservative treatment of radial tunnel syndrome is generally successful. Fixing the problem means limiting excessive or repetitive wrist movements, especially extension and rotation. In severe cases, a splint may be necessary to limit your motion. Try to avoid compression of your forearm, particularly from tight bands or braces. Use of a tennis elbow brace will likely aggravate your symptoms. You may find relief by applying ice or ice massage to the area for 10-15 minutes at a time.

 When you flex your elbow, the ulnar nerve is required to both stretch and slide through your cubital tunnel. If your ulnar nerve is “stuck” in the tunnel and does not glide when you flex your elbow, this leads to traction and irritation of the nerve. This is called “cubital tunnel syndrome.” The nerve may also be irritated from direct compression, like leaning your elbow on the edge of a desk or from arthritic spurs. Cubital tunnel syndrome is the second most common nerve compression problem in the arm, behind carpal tunnel syndrome.
When you flex your elbow, the ulnar nerve is required to both stretch and slide through your cubital tunnel. If your ulnar nerve is “stuck” in the tunnel and does not glide when you flex your elbow, this leads to traction and irritation of the nerve. This is called “cubital tunnel syndrome.” The nerve may also be irritated from direct compression, like leaning your elbow on the edge of a desk or from arthritic spurs. Cubital tunnel syndrome is the second most common nerve compression problem in the arm, behind carpal tunnel syndrome.