Here is a great exercise that targets those upper back and shoulder muscles.
Reverse Butterfly’s – Keep in mind that all of the work in this exercise is done by your shoulder blades. Your arms are just along for the ride.
Here is a great exercise that targets those upper back and shoulder muscles.
Reverse Butterfly’s – Keep in mind that all of the work in this exercise is done by your shoulder blades. Your arms are just along for the ride.
Your shoulder is formed by three bones; the scapula (shoulder blade), the clavicle (collar bone), and the humerus (long arm bone.) These bones come together to form a shallow ball & socket that relies upon the surrounding muscles for support. All of your shoulder muscles must work in a coordinated fashion to have a healthy and stable joint. Disruption of the normal rhythm of your shoulder blade creates abnormal strain on your shoulder and rotator cuff called “Scapular dyskinesis”. This dysfunction crowds the area of your shoulder where your rotator cuff tendons live and may create a painful pinching of your tendons or bursa each time you raise your arm. Many shoulder problems, including sprains/strains, tendinitis, bursitis, or rotator cuff irritation, result from this often overlooked culprit.

Although scapular dyskinesis can cause a variety of shoulder problems, it may initially go unnoticed. Up to 75% of healthy college athletes show some form of abnormal shoulder blade movement. If the condition is left untreated, you may begin to notice pain near the top of your shoulder. Sometimes the discomfort can radiate toward your neck or into your arm. Patients will often complain of a tender spot on the front of their shoulder. Long-standing altered mechanics can lead to bigger problems, including rotator cuff injury, shoulder instability, and arthritis.
The good news is that we have recognized the underlying cause of your shoulder problems and have treatments to correct it. You will need to perform your exercises consistently. You should also be conscious of your posture and try to avoid sitting or standing in “slouched” positions, as this is known to aggravate your problem.
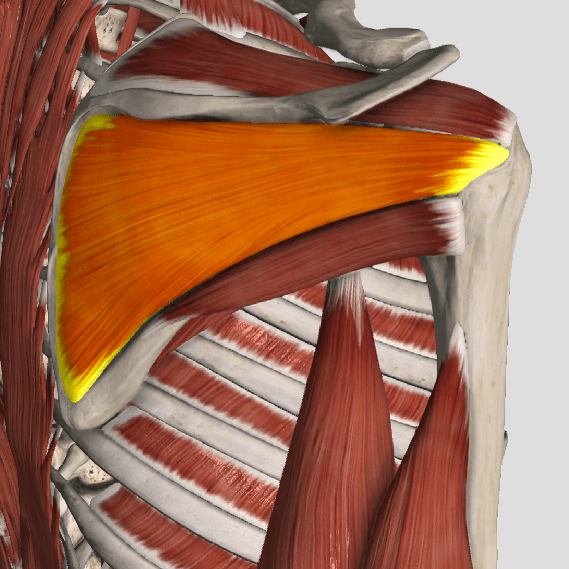
The supraspinatus is a muscle of the rotator cuff. Is sits above the infraspinatus and originates on the supraspinous fossa of the scapula. It’s insertion point is the superior facet of the greater tubercle of the humerus. It’s main function is to abduct the arm at the glenohumeral joint working with the deltoid. All rotator cuff muscles act to secure and support the head of the humerus in the glenoid fossa during arm movements acting as a sling. This muscle often gets impinged during overhead movements such as painting a ceiling. When trigger points form in this muscle they primarily refer a deep achy pain into the mid deltoid area with spillover pain radiating down the arm into the elbow.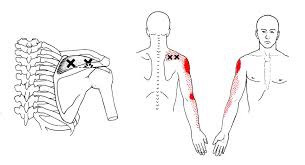
The tricep muscle is named for its three heads long, medial, and lateral. The long head originates on the infraglenoid tubercle, the medial head on the posterior humerus, and the lateral head on the posterior humerus as well. They join together to insert on the Olecranon process of the ulna. The triceps function to extend the elbow. Strong extension under resistance can cause trigger points to form. Pain referred from triceps trigger points can be felt in the posterior shoulder and down the posterior forearm, as well as in in the olecranon process and the lateral epicondyle which can cause “tennis elbow” pain.
A large number of factors have been identified as causes of trigger point activation. These include acute or chronic overload of muscle tissue, disease, psychological distress, systemic inflammation, homeostatic imbalances, direct trauma, radiculopathy, infections, and lifestyle choices such as smoking. Trigger points form as a local contraction of muscle fibres in a muscle or bundle of muscle fibres. These can pull on ligaments and tendons associated with the muscle which can cause pain to be felt deep inside a joint. It is theorized that trigger points form from excessive release of acetylcholine causing sustained depolarization of muscle fibres. Trigger points present an abnormal biochemical composition with elevated levels of acetylcholine, noradrenaline and serotonin and a lower ph. The contracted fibres in a trigger point constricts blood supply to the area creating an energy crisis in the tissue that results in the production of sensitizing substances that interact with pain receptors producing pain. When trigger points are present in a muscle there is often pain and weakness in the associated structures. These pain patterns follow specific nerve pathways that have been well mapped to allow for accurate diagnosis or the causative pain factor.

Your posture plays an important role in your overall health. Poor posture leads to chronic strain and discomfort. “Upper crossed syndrome” describes poor posture that results from excessive tightness in your shoulders and chest with weakness in your neck and mid-back. This combination forces your shoulders to roll inward and your head to project forward.
To help understand how upper crossed syndrome causes trouble, think of your spine as a telephone pole and your head as a bowling ball that sits on top. When the bowling ball is positioned directly over the top of the upright post, very little effort is required to keep it in place. If you tip the post forward and the ball begins to roll over the edge of the post, significantly more effort would be required from the muscles trying to hold it there. This effort results in chronic strain of the muscles of your neck and upper back.
The chronic strain is uncomfortable and may also lead to neck pain, upper back pain, headaches, TMJ pain, and ultimately- arthritis. This postural problem is exceptionally common in computer workstation users.
Correction of this problem is accomplished by stretching the tight muscles, strengthening weak muscles, and modifying your workstation. Treatment is aimed at reducing and eliminating symptoms through the use of Chiropractic adjustments, soft tissue release, acupuncture and trigger point therapy.
Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
The Bicep Brachii is perhaps the most recognizable muscle in the body. It’s the muscle that is most often flexed when someone says ” show me your muscles”. It is composed of two heads, the long head and the short head. The short head originates on the coracoid process of the scapula, and the long head on the supraglenoid tubercle. Both heads merge to insert on the radial tuberosity and bicipital aponeurosis into the deep fascia on the medial part of the forearm. The main actions of this muscle are elbow flexion and forearm supination(rotation with the palm of the hand going upward). This muscle also assists shoulder flexion. Trigger points in this muscle mainly refer pain into the shoulder, with spillover into the posterior aspect above the scapula. A less common referral is into the anterior elbow and forearm. 
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
One of the most common causes of shoulder pain is a rotator cuff (RC) tear. To determine just how common this is, one study looked at a population of 683 people regardless of whether or not they had shoulder complaints. There were 229 males and 454 females for a total of 1,366 shoulders. (The participants’ average age was 58 years, ranging from 22 to 87 years old.)
The research team found 20.7% had full thickness rotator cuff tears. Of those with shoulder pain, only 36% had tears found on ultrasound. Of those without shoulder pain, 17% also had tears! Risk factors for an increased for tearing of the rotator cuff include a history of trauma, the dominant arm (ie your right arm if you’re right handed), and increasing age.
In a review of radiologic studies of 2,553 shoulders, researchers found full-thickness rotator cuff tears in 11.75% and partial thickness tears in 18.49% of the subjects for a total of 30.24% having some degree of tearing. In this group, about 40% of tears were found in pain-free shoulders. The researchers concluded that rotator cuff tears are common and frequently asymptomatic.
Both of these studies support the necessity to FIRST consider the patient’s clinical presentation and then correlate that with the imaging results. In other words, the presence of a RC tear on an image (usually MRI or ultrasound) does NOT necessarily mean there is pain (and vise versa)!
So what other things could be causing the shoulder pain? There are many: impingement, tendonitis, bursitis, muscle strain, capsular (and other ligament) sprain, frozen shoulder, and osteoarthritis (the “wearing out” type). Also, rheumatoid arthritis, lupus, polymyalgia rheumatica and other autoimmune types of “arthropathies,” fibromyalgia, a herniated cervical disk, shoulder dislocations, whiplash injuries, and more!
Most importantly, we must NOT forget to include referred pain to the shoulder from an impaired heart (such as coronary heart disease or heart attack), lung, liver, or gall bladder as these problems commonly refer pain to the shoulder and may represent a MEDICAL EMERGENCY!