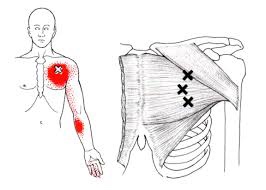
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Posture
Lumbar Spine Stabilization

This is a great way to increase the stability of your lower back.
- Lie with your stomach over a therapeutic ball while stabilizing yourself with your feet and arms and keep your head in line with your body.
- Tighten your abdominal muscles to flatten the spine by pulling your belly button towards your back and hold the contraction throughout the exercise.
- Bend one knee and lift it up towards the ceiling.
- Lower the leg and repeat on the other side.
Trigger points in the rhomboid muscles.
This is another common muscle to get trigger points. It originates on the spinous processes of the T2-T5 vertebrae. It inserts on the medial border of the scapula. It’s main actions are to adduct the scapula pulling it back toward the spine, and to rotate the glenohumeral joint downward. This muscle also prevents wining of the scapula. This muscle is often overloaded by a sitting posture where the shoulders are rolled forward such as when using a computer. The Rhomboids are often weak and under trained in people. Trigger points in this muscle cause pain and ache in the upper back between the shoulder blade. Strength trading for this muscle is necessary to help prevent postural overload. 
Trigger points in the trapezius muscle.
The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
How long does Whiplash last?

First, what is whiplash? It’s a lot of things, which is why the term WAD or Whiplash Associated Disorders has become the most common term for the main signs and symptoms associated with a whiplash injury. WAD is usually associated with a motor vehicle collision, but sports injuries, diving accidents, and falls are other common ways to sustain a WAD injury.
To answer the question of the month, in most cases, the recovery rate is high and favors those who resume their normal daily activities. The worse thing you can do when you sustain a WAD injury is to not do anything! Too much rest and inactivity leads to long-term disability. Of course, this must be balanced with the degree of injury, but even when the injury requires some “down time,” stay as active as possible during the healing phase.
Many people recover within a few days or weeks while a smaller percentage require months and about 10% may only partially recover. So what can be done to give you the best possible chance to fully recover as soon as possible?
During recovery, you can expect your condition to fluctuate in intensity so “listen” to your body, let it “guide” you during activity and exercise, and stay within “a reasonable boundary of pain” during your activity. Remember, your best chance for full recovery FAVORS continuing a normal lifestyle. Make reasonable modifications so you can work, socialize, and do your “normal” activities!
The KEY: Stay in control of your condition – DO NOT let it control you! Here are some tips:
1) POSTURE CONTROL: Keep the weight of the head back by gliding your chin back until you “hit” a firm end-point. Then release it slightly so it’s comfortable—this is your NEW head position!
2) FLEXIBILITY: Try this range of motion (ROM) exercise… Slowly flex your neck forwards and then backwards, then bend your neck to the left and then the right, and then rotate it to the left and to then to the right. THINK about each motion and avoid sharp, knife-like pain; a “good-hurt” is okay! Next, do the same thing with light (one-finger) resistance in BOTH directions. Try three slow reps four to six times a day!
3) MUSCLE STRENGTH: Try pushing your head gently into your hand in the six directions listed above to provide a little resistance. Next, reach back with both hands or wrap a towel around your neck and pull forwards on the towel while you push the middle of your neck backwards into the towel doing the chin-tuck/glide maneuver (same as #1). Repeat three to five times slowly pushing, and more importantly, release the push slower! This is the MOST IMPORTANT of the strengthening exercises in most cases! Next, “squeeze” your shoulder blades together followed by spreading them as far apart as possible (repeat three to five times).
4) PERIODIC BREAKS: Set a timer to remind yourself to do a stretch, get up and move, to tuck your chin inwards (#1) and do some of #2 and #3 every 30-60 minutes.
5) LIFTING/CARRYING/WORK: Be SMART! Do not re-injure yourself. Change the way you handle yourself in your job, in the house, and while performing recreational activities.
6) HOUSEHOLD ACTIVITIES: Use a dolly to move boxes and keep commonly used items within easy reach (not too high or low).
Be smart, stay educated, work within the range your body tells you is “safe” and most importantly, STAY IN CONTROL!!!
Trigger points in the Levator scapula
The Levator scapula is a muscle in your neck that originates on the transverse processes of C1-C4 and inserts on the superior part of the medial border of the scapula. The primary actions of this muscle are to elevate the scapula and rotate the glenoid fossa downward. It also rotates the neck to the same side and assists in extension. When this muscle is tight it restricts neck rotation resulting in the classic “stiff neck”. With a forward head position the Levator is often stretched and over worked. To help combat this you must get the head back by releasing the anterior chest and neck muscles. Trigger points in this muscle refer pain into the angle of the neck and down the shoulder blade.
Hip Abductor Weakness

* The gluteus medius contributes approximately 70% of the abduction force required to maintain pelvic leveling during single leg stance.
* Hip abductor strength is the single greatest contributor to lower extremity frontal plain alignment during activity.
* There is no “typical” presentation for hip abductor weakness, but the problem must be considered in any patient with lower chain symptomatology, particularly those with hip tendinopathy, greater trochanteric pain syndrome, iliotibial band syndrome, patellofemoral pain syndrome, ACL injury, medial knee pain, and lower back pain.
*Hip abductor weakness is often accompanied by lower crossed syndrome – a larger pattern of biomechanical dysfunction involving weakness of the abdominal wall and hypertonicity in the hip flexors and paraspinal musculature. Evaluation should include a relatively global assessment of lumbopelvic muscle and joint function. Additionally, clinicians should assess for the presence of foot hyperpronation in patients with hip abductor weakness.
Referenced from:
ChiroUp.com “Hip Abductor Weakness Clinical Pearls
Workstation Ergonomics
Ergonomics is the science of adjusting your workstation to minimize strain in the following ways:
✓ Maintain proper body position and alignment while sitting at your desk – Hips, knees and elbows at 90 degrees, shoulders relaxed, feet flat on floor or footrest.
✓ Wrists should not be bent while at the keyboard. Forearms and wrists should not be leaning on a hard edge.
✓ Use audio equipment that keeps you from bending your neck (i.e., Bluetooth, speakerphones, headsets).
✓ Monitors should be visible without leaning or straining and the top line of type should be 15 degrees below eye level.
✓ Use a lumber roll for lower back support.
✓ Avoid sitting on anything that would create an imbalance or uneven pressure (like your wallet).
✓ Take a 10-second break every 20 minutes: Micro activities include: standing, walking, or moving your head in a “plus sign” fashion.
✓ Periodically, perform the “Brugger relief position” (See video below) -Position your body at the chair’s edge, feet pointed outward. Weight should be on your legs and your abdomen should be relaxed. Tilt your pelvis forward, lift your sternum, arch your back, drop your arms, and roll out your palms while squeezing your shoulders together. Take a few deep cleansing breaths.
Trigger points in the masseter muscle

The masseter is the main muscle that moves your jaw. It originates on the zygomatic arch and maxilla, and inserts on the coronoid process and Ramus of the mandible. It’s actions are to elevate the mandible and close the jaw. The deep fibres of this muscle also retrude the mandible. This muscle commonly harbours trigger points as a result of teeth grinding. Trigger points in this muscle are often also associated with tmj dysfunction. Trigger points in the upper part of this muscle will refer pain to the upper molars and maxilla often felt as sinusitis. Trigger points in the lower portion of this muscle refer to the lower molars and temple. All trigger points can cause tooth sensitivity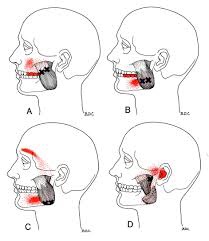
Up Close & Personal With Headaches.

Headaches are REALLY common! In fact, two out of three children will have a headache by the time they are fifteen years old, and more than 90% of adults will experience a headache at some point in their life. It appears safe to say that almost ALL of us will have firsthand knowledge of what a headache is like sooner or later!
Certain types of headaches run in families (due to genetics), and headaches can occur during different stages of life. Some have a consistent pattern, while others do not. To make this even more complicated, it’s not uncommon to have more than one type of headache at the same time!
Headaches can vary in frequency and intensity, as some people can have several headaches in one day that come and go, while others have multiple headaches per month or maybe only one or two a year. Headaches may be continuous and last for days or weeks and may or may not fluctuate in intensity.
For some, lying down in a dark, quiet room is a must. For others, life can continue on like normal. Headaches are a major reason for missed work or school days as well as for doctor visits. The “cost” of headaches is enormous—running into the billions of dollars per year in the United States (US) in both direct costs and productivity losses. Indirect costs such as the potential future costs in children with headaches who miss school and the associated interference with their academic progress are much more difficult to calculate.
There are MANY types of headaches, which are classified into types. With each type, there is a different cause or group of causes. For example, migraine headaches, which affect about 12% of the US population (both children and adults), are vascular in nature—where the blood vessels dilate or enlarge and irritate nerve-sensitive tissues inside the head. This usually results in throbbing, pulsating pain often on one side of the head and can include nausea and/or vomiting. Some migraine sufferers have an “aura” such as a flashing or bright light that occurs within 10-15 minutes prior to the onset while other migraine sufferers do not have an aura.
The tension-type headache is the most common type and as the name implies, is triggered by stress or some type of tension. The intensity ranges between mild and severe, usually on both sides of the head and often begin during adolescence and peak around age 30, affecting women slightly more than men. These can be episodic (come and go, ten to fifteen times a month, lasting 30 min. to several days) or chronic (more than fifteen times a month over a three-month period).
There are many other types of headaches that may be primary or secondary—when caused by an underlying illness or condition. The GOOD news is chiropractic care is often extremely helpful in managing headaches of all varieties and should be included in the healthcare team when management requires a multidisciplinary treatment approach.
Most of know someone who has been affected by headaches. If they are looking for help and information please feel free to contact us at 204-586-8424 or at info@aberdeenchiropractic.com.
