Whiplash is really a slang term for the rapid back and forth whipping of the head on the neck, usually associated with motor vehicle accidents. The title “Whiplash Associated Disorders”, or WAD, describes it best because it includes ALL of the MANY signs and symptoms of the disorder.
WAD basically comes in three sizes based on the degree of injury. A WAD I is present when there is pain but no physical examination findings; WAD II occurs when there are exam findings but no neurological loss (numbness or weakness); and WAD III includes loss of neurological function. There is also a separate WAD level that includes fractures and dislocations (WAD IV).
There are many things that can be done by the patient to assist in the healing process for WAD. The first well-studied recommendation is to “continue with your usual activities.” Try to keep active and not change your routine. The good news is that WAD (especially types I and II) usually resolves without complication, and recovery is even more likely to occur if you don’t deviate much from your routine.
For those whose symptoms are more severe and/or not resolving, mobilization and manipulation of the neck and back are very effective treatment options. In addition to treatments you’d receive in a chiropractic office, there are MANY things you can do at home as “self-help strategies.” Some of these include (“PRICE”):
1) PROTECT: Though it’s important to continue with your usual daily activities, this is dependent on both the degree of tissue injury and your pain tolerance. So do as many of your usual daily activities as possible, but AVOID those that result in a sharp, lancinating type of pain or those where recovery from the pain is delayed. Therefore, this category may require modifying your ADLs (activities of daily living). A cervical collar (hard orsoft) should NOT to be used UNLESS you have an unstable injury (fracture or a grade III sprain).
2) REST: Doing too much is like picking at a cut (which can delay healing) and doing too little can lead to a delayed healing response as well. Staying within reasonable pain boundaries is a good guide.
3) ICE > HEAT: Ice reduces swelling, and your doctor will typically recommend it over applying heat, especially on a recent injury. Heat draws fluids in, and while it may feel good, it can make your symptoms worse.
4) COMPRESS: We can basically ignore this when referencing neck pain. This pertains better to wrapping an ankle, knee, wrist, or elbow with an elastic compression orthotic or brace.
5) ELEVATE: This too is meant for the acute stages of an extremity injury like a foot or ankle.
Exercises unique for neck pain in the acute, subacute, and chronic stages of healing are perhaps the most important of the self-help approaches. In the ACUTE phase, try these…
1) Range of Motion: Once again, stay within “reasonable pain boundaries” as you move your head forwards, backwards, side to side, and rotate left and right. These can be done either with or without LIGHT resistance applied using one or two fingers placed against your head. Limit the repetitions to three slow reps in each direction and emphasize the release of the movement.
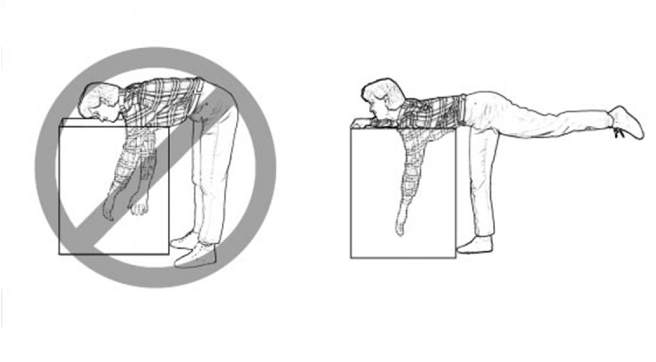
2) Chin/head Glides: Tuck in the chin (think of creating a double or triple chin) followed by poking the chin/head out.
In the SUBACUTE and CHRONIC phases of healing, the importance of strengthening the deep neck flexors cannot be over emphasized. Please refer to last week’s article for a description of this (see #3 of the 6 recommendations listed).