Diagnosis of trigger points typically takes into account symptoms, pain patterns, and manual palpation. When palpating the therapist will feel for a taut band of muscle with a hard nodule within it. Often a local twitch response will be elicited by running a finger perpendicular to the muscle fibres direction. Pressure applied to the trigger point will often reproduce the pain complaint of the patient and the referral pattern of the trigger point. Often there is a heat differential in the local area of the trigger point. 
Pain
Trigger points in the biceps Brachii muscle.
The Bicep Brachii is perhaps the most recognizable muscle in the body. It’s the muscle that is most often flexed when someone says ” show me your muscles”. It is composed of two heads, the long head and the short head. The short head originates on the coracoid process of the scapula, and the long head on the supraglenoid tubercle. Both heads merge to insert on the radial tuberosity and bicipital aponeurosis into the deep fascia on the medial part of the forearm. The main actions of this muscle are elbow flexion and forearm supination(rotation with the palm of the hand going upward). This muscle also assists shoulder flexion. Trigger points in this muscle mainly refer pain into the shoulder, with spillover into the posterior aspect above the scapula. A less common referral is into the anterior elbow and forearm. 
What is a trigger point
Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
Do I have a cuff tear?
One of the most common causes of shoulder pain is a rotator cuff (RC) tear. To determine just how common this is, one study looked at a population of 683 people regardless of whether or not they had shoulder complaints. There were 229 males and 454 females for a total of 1,366 shoulders. (The participants’ average age was 58 years, ranging from 22 to 87 years old.)
The research team found 20.7% had full thickness rotator cuff tears. Of those with shoulder pain, only 36% had tears found on ultrasound. Of those without shoulder pain, 17% also had tears! Risk factors for an increased for tearing of the rotator cuff include a history of trauma, the dominant arm (ie your right arm if you’re right handed), and increasing age.
In a review of radiologic studies of 2,553 shoulders, researchers found full-thickness rotator cuff tears in 11.75% and partial thickness tears in 18.49% of the subjects for a total of 30.24% having some degree of tearing. In this group, about 40% of tears were found in pain-free shoulders. The researchers concluded that rotator cuff tears are common and frequently asymptomatic.
Both of these studies support the necessity to FIRST consider the patient’s clinical presentation and then correlate that with the imaging results. In other words, the presence of a RC tear on an image (usually MRI or ultrasound) does NOT necessarily mean there is pain (and vise versa)!
So what other things could be causing the shoulder pain? There are many: impingement, tendonitis, bursitis, muscle strain, capsular (and other ligament) sprain, frozen shoulder, and osteoarthritis (the “wearing out” type). Also, rheumatoid arthritis, lupus, polymyalgia rheumatica and other autoimmune types of “arthropathies,” fibromyalgia, a herniated cervical disk, shoulder dislocations, whiplash injuries, and more!
Most importantly, we must NOT forget to include referred pain to the shoulder from an impaired heart (such as coronary heart disease or heart attack), lung, liver, or gall bladder as these problems commonly refer pain to the shoulder and may represent a MEDICAL EMERGENCY!
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
Trigger points in the deltoid muscle.
The deltoid is the the muscle that is most often thought of as the “shoulder.” It is the diamond shaped muscle that caps the shoulder joint. It originates on the clavicle, the acromion, and the spine of the scapula. It inserts on the deltoid tuberosity of the humerus. As a whole unit the deltoid laterally abducts the humerus at the glenohumeral joint. The anterior portion of the delt forward flexes the arm, as well as horizontally flexing the arm across the chest. Since the deltoid is involved in almost all shoulder movements it is especially prone to trigger points. Points in the anterior deltoid refer into the anterior and lateral shoulder. Trigger points in the posterior deltoid refer pain into the posterior shoulder with spillover down the lateral arm. 
He barely hit me; why does it hurt?
Error
This video doesn’t exist
You may have heard the comment, “If there’s no damage to the car, then there’s no injury.” Unfortunately, that does not always seem to be the case.
There are MANY factors that affect the dynamics of a collision and whether or not injury occurs. A short list includes: vehicle type and design, speed, angle of collision, momentum, acceleration factors, friction, kinetic and potential energy, height, weight, muscle mass, seat back angle and spring, head position upon impact, etc.
Consider Sir Isaac Newton’s Third Law of Motion: “For every action there is an equal and opposite reaction.” This law applies to a car accident at any speed. Using the analogy of hitting a pool ball into the corner pocket straight on, when the cue ball stops, its momentum is transferred to the target ball which accelerates at the same speed…hopefully into the corner pocket!
This example is not quite the same as an automobile collision because the energy transfer is very efficient due in part to the two pool balls not deforming (crushing or breaking) on impact with one another. If either ball did deform, more energy absorption would occur and the acceleration of the second ball would be lower.
In fact, in the United States, vehicle bumpers are tested at 2.5 mph with impact equipment of similar mass with the test vehicle’s brakes disengaged and the transmission in neutral. National Highway Transportation Highway Safety Administration (NHTSA) vehicle safety standards demand that no damage should occur to the car in this scenario.
However, energy transfer occurs very quickly and with a greater amount of force when there is no vehicle deformation (damage). As a result, a greater amount of energy (described as G-force) is directly transferred to the occupants inside the vehicle—increasing the risk of injury. A 1997 Society of Automobile Engineers article provided an example in which the same 25 mph (12 m/s) collision resulted in a five-times greater force on the occupants of the vehicle when the crush distance of the impact fell from 1 meter to .2 meters.
So be aware that even low-speed impacts can still place quite a bit of force on your body, even if the bumper of your car doesn’t have a scratch on it.
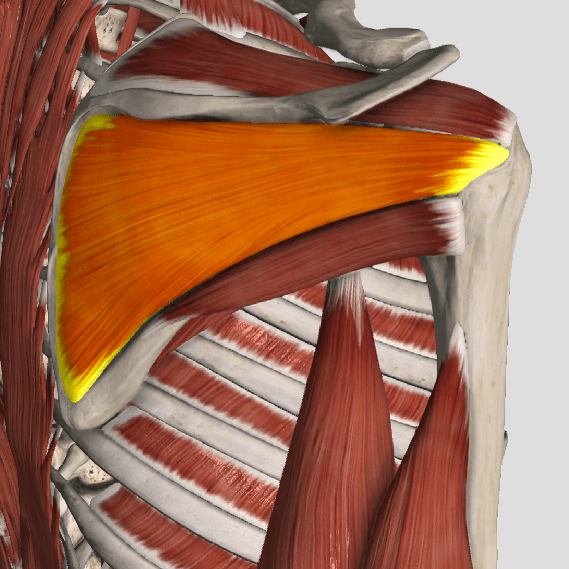
Trigger points in the pectoralis minor muscle.
The pectoralis minor is a small strap like muscle that is underneath (deep) to the pectoralis major. It originates on the third to fifth rib, near the costal cartilages. It’s insertion is on the coracoid process of the scapula. It acts to draw the scapula forward, downward, and inward at nearly equal angles ( think of rounding or shrugging your shoulders forward). This muscle is very often shortened and tight in people due to the high prevalence of desk jobs. This muscle pulls the shoulder blade forward resulting in the muscles in the back(rhomboid and mid traps) being chronically strained. Trigger points that form in the pec minor primarily refer pain over the anterior chest and shoulder, with spillover down the medial arm. Trigger points in the left side can mimic angina. 
What evidence do we have of whiplash?

Whiplash, or WAD (Whiplash Associated Disorders), refers to a neck injury where the normal range of motion is exceeded, resulting in injury to the soft-tissues (hopefully with no fractures) in the cervical region. There are a LOT of factors involved that enter into the degree of injury and length of healing time. Let’s take a closer look!
Picture the classic rear-end collision. The incident itself may be over within 300 milliseconds (msec), which is why it’s virtually impossible to brace yourself effectively for the crash as a typical voluntary muscle contraction takes two to three times longer (800-1000 msec) to accomplish.
In the first 50 msec, the force of the rear-end collision pushes the vehicle (and the torso of the body) forwards leaving the head behind so the cervical spine straightens out from its normal “C-shape” (or lordosis). By 75-100 msec, the lower part of the neck extends or becomes more C-shaped while the upper half flexes or moves in an opposite direction creating an “S” shape to the neck. Between 150-200msec, the whole neck hyper extends and the head may hit the head rest IF the headrest is positioned properly. In the last 200-300 msec, the head is propelled forwards into flexion in a “crack the whip” type of motion.
Injury to the neck may occur at various stages of this very fast process, and many factors determine the degree of injury such as a smaller car being hit by a larger car, the impact direction, the position of the head upon impact (worse if turned), if the neck is tall and slender vs. short and muscular, the angle and “springiness” of the seat back and relative position of the headrest, dry vs. wet/slippery pavement, and airbag deployment, just to name a few.
Some other factors that can predict recovery include: limited neck motion, the presence of neurological loss (nerve specific muscle weakness and/or numbness/tingling), high initial pain levels (>5/10 on a 0-10 scale), high disability scores on questionnaires, overly fearful of harming oneself with usual activity and/or work, depressive symptoms, post-traumatic stress, poor coping skills, headaches, back pain, widespread or whole body pain, dizziness, negative expectation of recovery, pending litigation, catastrophizing, age (older is worse), and poor pre-collision health (both mental and physical).
Research shows the best outcomes occur when patients are assured that most people fully recover and when patients stay active and working as much as possible. Studies have shown it’s best to avoid prolonged inactivity and cervical collars unless under a doctor’s orders. It’s also a good idea to gradually introduce exercises aimed at improving range of motion, postural endurance, and motor control provided doing so keeps the patient within reasonable pain boundaries. Chiropractic manipulation restores movement in fixed or stuck joints in the back and neck and has been found to help significantly with neck pain and headaches, particularly for patients involved in motor vehicle collisions. A doctor of chiropractic may also recommend using a cervical pillow, home traction, massage, and other therapies as part of the recovery process.
It is important to be aware that fear of normal activity and not engaging in usual activities and work can delay healing and promote chronic problems and long-term disability. It’s suggested patients avoid opioid medication use due to the addictive problems with such drugs. Ice and anti-inflammatory herbs or nutrients (like ginger, turmeric, and bioflavonoids) are safer options. Your doctor of chiropractic can guide you in this process!
Have you Been Told You Have TMJ Disorder?
Temporomandibular Disorder (TMD) is a term used to describe a group problems that cause pain in the temporomandibular joint, also called the TMJ. These problems can arise from the muscles around the joint, the disc within the joint or the bony portion of the joint itself. Imbalances between the muscles that open and close your jaw are the most common culprit.

Up to 25% of the population will suffer with TMD symptoms. Most patients are 20-50 years old and the condition is 2-3 times more common in females. Typical symptoms include: jaw clicking, limited mouth opening, possible jaw locking and pain. Chewing and eating usually make your symptoms more noticeable. TMD pain is generally described as an “ache” located in front of your ear canal but may also refer to other areas of your face, head, neck and shoulders. TMD patients often suffer from headaches.
TMD is more common in people who clench their jaw or grind their teeth, especially at night. Bad posture and emotional stress are contributors to this problem. You are three times more likely to suffer with TMD if you have been involved in a “whiplash” accident.
Conservative treatments, like those provided by our office, have been shown to be as effective as any surgery for most patients with TMD. Treatment is simple, focusing on “massaging” tightness out of the jaw muscles, restoring movement to any restricted joints (including your neck and upper back), and prescribing exercises to improve flexibility.
You should avoid aggravating activities like chewing gum or eating “rubbery” foods. Limit excessive talking. A custom fitted mouth guard may be prescribed to help minimize grinding & clenching and promote relaxation of your jaw muscles at night. Patients with night-time symptoms should avoid stressful activity before bedtime and try to sleep in a “neutral” position. In some cases, stress management techniques, like biofeedback, can assist you in learning how to relax your jaw muscles.
