Dr Janet travel coined the term trigger point in 1942 to describe clinical findings with characteristics of pain related a discrete irritable point in muscle or fascia that was not caused by acute trauma, inflammation, degeneration, neoplasm or infection. The painful point can be palpated as a nodule or tight band in the muscle that can produce a local twitch response when stimulated. Palpation of the trigger point reproduces the pain and symptoms of the patient and the pain radiates in a predictable referral pattern specific to the muscle harbouring the trigger point.
Overuse Injury
What to expect with a trigger point massage.
A treatment with Bryan is very user friendly. And, no, you don’t have to remove any clothing. However, bringing a t-shirt and a pair of shorts or sweats is recommended.

The first time you come for a treatment you will be asked to fill out a Client History form. Bryan will go over the information you provide, asking for more detail and discussing the type of pain you are having and its location.
The treatment itself involves locating the Trigger Points in the muscle or soft tissue and applying a deep focused pressure to the Point. This will reproduce the pain and the referral pattern that is characteristic of that pain.
The treatment will be uncomfortable at first, but as the Trigger Points release, the pain will decrease. The pressure will always be adjusted to your tolerance level. If, at any time, you feel too uncomfortable you can ask Bryan to ease off a bit.
Depending on your specific problem, Bryan may also use some stretching and / or range-of-motion techniques, as needed.
After treatment, it is usually recommended that the client apply moist heat to the area treated.
Trigger points in the deltoid muscle.
The deltoid is the the muscle that is most often thought of as the “shoulder.” It is the diamond shaped muscle that caps the shoulder joint. It originates on the clavicle, the acromion, and the spine of the scapula. It inserts on the deltoid tuberosity of the humerus. As a whole unit the deltoid laterally abducts the humerus at the glenohumeral joint. The anterior portion of the delt forward flexes the arm, as well as horizontally flexing the arm across the chest. Since the deltoid is involved in almost all shoulder movements it is especially prone to trigger points. Points in the anterior deltoid refer into the anterior and lateral shoulder. Trigger points in the posterior deltoid refer pain into the posterior shoulder with spillover down the lateral arm. 
Another tunnel injury? Seriously?
Your radial nerve begins in your neck and travels past your elbow en route to its final destination in your hand. Just beyond your elbow, this nerve passes through a 2-inch area on the back of your forearm called the “Radial tunnel”. “Radial tunnel syndrome” means that your radial nerve has been compressed or irritated within this space-leading to forearm pain or hand weakness.

Radial tunnel syndrome is thought to result from muscular overuse, especially prolonged or excessive wrist extension or rotation. The most common cause of compression comes from excessive tightness in a muscle called the “Supinator”. Workers whose jobs require heavy or repetitive wrist movements are at an increased risk for this disorder. Occasionally, the radial nerve can become irritated from direct compression by a tight band or brace. The condition may be more common in those who have diabetes or thyroid problems.
Symptoms from irritation of the radial nerve depend upon which specific nerve fibers are irritated. The most common symptoms include pain, numbness, tingling or decreased sensitivity along the top of your forearm radiating toward your hand and thumb. The symptoms often mimic those of “tennis elbow.” When the nerve fibers that control muscle function become compressed, you may experience weakness when trying to extend your fingers, hand or wrist. Seventy percent of radial tunnel patients also have problems in their neck or upper back.
Conservative treatment of radial tunnel syndrome is generally successful. Fixing the problem means limiting excessive or repetitive wrist movements, especially extension and rotation. In severe cases, a splint may be necessary to limit your motion. Try to avoid compression of your forearm, particularly from tight bands or braces. Use of a tennis elbow brace will likely aggravate your symptoms. You may find relief by applying ice or ice massage to the area for 10-15 minutes at a time.
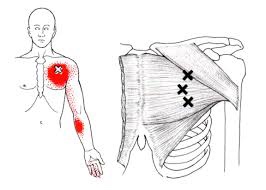
Trigger points in the pectoralis minor muscle.
The pectoralis minor is a small strap like muscle that is underneath (deep) to the pectoralis major. It originates on the third to fifth rib, near the costal cartilages. It’s insertion is on the coracoid process of the scapula. It acts to draw the scapula forward, downward, and inward at nearly equal angles ( think of rounding or shrugging your shoulders forward). This muscle is very often shortened and tight in people due to the high prevalence of desk jobs. This muscle pulls the shoulder blade forward resulting in the muscles in the back(rhomboid and mid traps) being chronically strained. Trigger points that form in the pec minor primarily refer pain over the anterior chest and shoulder, with spillover down the medial arm. Trigger points in the left side can mimic angina. 
Trigger points in the pectoralis Major muscle.
The pectoralis major or “pecs” is commonly thought of as the chest muscle. It originates on the clavicle, sternum, costal cartilage , and the external oblique aponeurosis. It inserts on the intertubercular groove of the humerus. Its main actions are to adduct the shoulder and to internally rotate the humerus. This muscle gets chronically shortened by a rounded shoulder forward posture such as from prolonged sitting. Tightness in this muscle can cause strain in the rhomboids and traps. When trigger points form in this muscle they refer pain into the anterior shoulder, as well as the anterior chest and medial aspect of the arm. Trigger points in the pecs can also cause nipple hypersensitivity. Trigger points in the left pec muscle can mimic heart pain.
Trigger points in the rhomboid muscles.
This is another common muscle to get trigger points. It originates on the spinous processes of the T2-T5 vertebrae. It inserts on the medial border of the scapula. It’s main actions are to adduct the scapula pulling it back toward the spine, and to rotate the glenohumeral joint downward. This muscle also prevents wining of the scapula. This muscle is often overloaded by a sitting posture where the shoulders are rolled forward such as when using a computer. The Rhomboids are often weak and under trained in people. Trigger points in this muscle cause pain and ache in the upper back between the shoulder blade. Strength trading for this muscle is necessary to help prevent postural overload. 
Workers compensation cases highlight the value of chiropractic care

A newly published analysis of 5511 workers compensation cases highlights the value of chiropractic care: “those injured workers who first saw a chiropractor experienced shorter first episodes of compensation (vs. physical therapy alone)”.
If you or someone you know has suffered a job-related injury, call us today. Our goal is to provide the most effective care that gets you back to work ASAP!
Trigger points in the trapezius muscle.
The trapezius muscle is a large diamond shaped muscle in you mid/upper back and neck. This muscle is one of the most common sites where trigger points can form. This muscle originates on the Nuchal ligament and the spinous processes of C6-T12. It inserts on the spine of the scapula, the acromion process, and the distal clavicle. The upper fibres elevate the shoulder and rotate the glenoid fossa (shoulder socket) upward. The lower fibres assist this motion as well as help depress the shoulder. The middle fibres of this muscle strongly adduct the scapula. This muscle is susceptible to postural overload such as sitting at desk all day. Trigger points on the lateral upper edge refer into the lateral neck and temples, causing “tension neck ache”as well as headache pain.Trigger points in the middle and lower fibres refer pain into the posterior neck and shoulder. 
Our Condition of the Month: ITB Syndrome
Iliotibial Band Syndrome
Your iliotibial band is a fibrous band of tissue running from the crest of your hip, down to your knee. A muscle near the crest of your hip called the tensor fascia lata, attaches to this band to help control movements of your leg. Your iliotibial band passes over the point of your hip and over another bony bump on the outside of your knee called the lateral epicondyle. When the band is too tight, it can become painfully inflamed as it repeatedly rubs over the top of either of these bony projections. Irritation at the bony bump near the knee is called iliotibial band friction syndrome.
The condition usually presents as pain on the outside of your knee that becomes worse with repetitive knee flexion or extension. This condition is the leading cause of lateral knee pain in runners, especially slower “joggers.” The pain usually develops 10-15 minutes into the workout. You may sometimes feel or hear a click during movement. Symptoms generally ease at rest. Running on slick “wintry” surfaces may aggravate the condition. Excessively worn running shoes may be a culprit.
This problem is commonly caused by weakness in your gluteal muscles. When these muscles are weak, the muscle that attaches to your iliotibial band must contract harder to stabilize your hip. Having one leg longer than another is a known aggravating factor.
Runners should minimize downhill running and avoid running on a banked surface like the crown of a road or indoor track, as well as wet or icy surfaces. Runners should reverse directions on a circular track at least each mile. Bicyclists may need to adjust seat height and avoid “toe in” pedal positions. Avoid using stair climbers or performing squats and dead lifts. Sports cream and home ice massage may provide some relief of symptoms.
