The adductor longus is a muscle of the groin. It originates on the pubic body just below the pubic crest, and inserts on the middle third of the linea aspera of the femur. It acts on the hip joint to cause adduction and flexion. Distal Trigger points in this muscle refer pain to the upper medial knee and down the tibia. Proximal trigger points refer pain into the anterior hip. These trigger points are the most common muscular cause of groin pain. 
Knee Pain
What is Lumbar Stenosis?

The term stenosis means “narrowing” of a tube or opening. Spinal stenosis means that the tube surrounding your spinal cord and nerve roots has become too small, and your nerves are being compressed. Stenosis can arise in different ways. Sometimes, people are born with a spinal canal that is too small. Other times, the canal may have been narrowed by surgery or conditions like disc bulges. Most commonly, spinal stenosis arises from chronic arthritic changes that narrow the canal. This type of stenosis usually develops slowly over a long period of time, and symptoms show up later in life.
Patients with stenosis often report pain, tingling, numbness or weakness in their legs. Lower back pain may or may not be present, but leg symptoms are usually more bothersome. You may notice increasing symptoms from standing or walking and relief while sitting because the available space in your spinal canal decreases when you stand, walk or lean back and increases when you sit or flex forward. Walking down hill is usually more uncomfortable than walking up hill. You may notice that when you walk with a shopping cart or lawn mower, you are more comfortable, as this promotes slight flexion. Sleeping on your side in a fetal position with a pillow between your knees may be most comfortable.
The natural course of spinal stenosis is variable. Most patients notice their symptoms stay about the same over time, while others are divided into fairly equal groups who either improve or worsen. Be sure to tell your doctor if you notice that your legs become cold, swollen or change color. Likewise, tell us if you notice a fever, unexplained weight loss, flu-like symptoms, excessive thirst or urination, numbness in your groin or loss of bladder control.
While there is no non-surgical cure for stenosis, we offer potent treatments to help ease your symptoms. Treatment is focused on helping improve your mobility so that you can walk and function better. You will be given exercises to help with conditioning. You should avoid activities that increase your pain, including heavy lifting or those that cause you to extend your back, like prolonged standing or overhead activity. When you are forced to stand, you may find relief by slightly elevating one foot on a stool or bar rail. You may find relief while washing dishes if you open your cabinet door and alternately rest one foot on the inside of the cabinet to provide a little bit of flexion. Recumbent cycling is often a more tolerable alternative to walking or running. Some patients report relief by using an inversion table.
Trigger points and fibromyalgia
Myofascial pain syndrome (trigger points) and fibromyalgia are often confused to be the same condition and while there is a lot of interrelatedness between the two they are not quite identical. The clinical definition of a trigger point is “a hyper irritable spot associated within a taut band of skeletal muscle that is painful on compression or muscle contraction, and usually responds with a referred pain pattern distant from the spot”. Trigger points form from an overload trauma to the muscle tissue. This is contrasted with fibromyalgia which is defined as “a medical condition characterized by chronic widespread pain and a heightened pain response to pressure. Other symptoms include tiredness to a degree that normal activities are affected, sleep problems and troubles with memory. Some people also report restless leg syndrome, bowel and bladder problems, numbness and tingling and sensitivity to noise, lights and temperature. It is also associated with depression, anxiety, and post traumatic stress disorder”. Fibromyalgia will also present with localized tender points which are often mistaken for trigger points. Where these two conditions become somewhat interrelated is via the nervous system. Fibromyalgia patients suffer from a super-sensitization of the nervous system causing hyperirritability and pain. Myofascial trigger points can be caused by,or be the cause of, super sensitization. An active trigger point will irritate the sensory nerves around it eventually leading to super-sensitization. Trigger points have also been showed to form of become active due to super-sensitization. Both of these conditions can perpetuate the other, leading to layers of pain and symptoms. This being the case, trigger point therapy can have a very positive effect on decreasing the severity of pain and symptoms in patients suffering from fibromyalgia.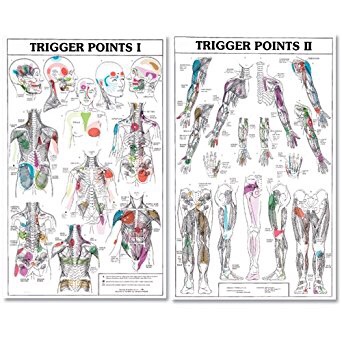

Trigger points in the adductor longus and brevis.
These muscles are located in the groin. The longus originates on the pubic body just below the pubic crest and inserts on the middle third of the linea aspera.The brevis muscle originates on the inferior ramus and body of the pubis and has its attachment to the lesser trochanter and linea aspera of the femur. Trigger points in these muscles are the most common muscular cause of groin pain. Distal trigger points refer pain to the upper medial knee and down the tibia. Proximal trigger points refer into the anterior hip area.
A weak lateral chain will stop you in your tracks.
One very important job of your hip muscles is to maintain the alignment of your leg when you move. One of the primary hip muscles, the gluteus medius, plays an especially important stabilizing role when you walk, run, or squat. The gluteus medius attaches your thigh bone to the crest of your hip. When you lift your left leg, your right gluteus medius must contract in order to keep your body from tipping toward the left. And when you are standing on a bent leg, your gluteus medius prevents that knee from diving into a “knock knee” or “valgus” position.
 Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
Weakness of the gluteus medius allows your pelvis to drop and your knee to dive inward when you walk or run. This places tremendous strain on your hip and knee and may cause other problems too. When your knee dives inward, your kneecap is forced outward, causing it to rub harder against your thigh bone- creating a painful irritation and eventually arthritis. Walking and running with a relative “knock knee” position places tremendous stress on the ligaments around your knee and is a known cause of “sprains”. Downstream, a “knock knee” position puts additional stress on the arch of your foot, leading to other painful problems, like plantar fasciitis. Upstream, weak hips allow your pelvis to roll forward which forces your spine into a “sway back” posture. This is a known cause of lower back pain. Hip muscle weakness seems to be more common in females, especially athletes.
You should avoid activities that cause prolonged stretching of the hip abductors, like “hanging on one hip” while standing, sitting crossed legged, and sleeping in a side-lying position with your top knee flexed and touching the bed. Patients with fallen arches may benefit from arch supports or orthotics. Obesity causes more stress to the hip muscles, so overweight patients may benefit from a diet and exercise program. The most important treatment for hip abductor weakness is strength training. Hip strengthening is directly linked to symptom improvement. Moreover, people with stronger hip muscles are less likely to become injured in the first place. The exercises listed below are critical for your recovery.
Meralgia paresthetica? Yeah, we know all about it.
Meralgia paresthetica is an often missed diagnosis for tingling, numbness, and burning pain on the front and outside of your thigh. The condition is caused by a pinching or irritation to the “lateral femoral cutaneous nerve” that supplies sensation to your thigh.
 This nerve can be compressed beneath a ligament, tendon or tight muscle in your hip and pelvis. Pregnancy or being even slightly overweight makes this condition more likely. Tight clothing including girdles, compressive shorts, or tight belts may aggravate or cause this condition. Carpenters’ tool belts or police duty belts may compress this nerve. Prolonged sitting or lying in a fetal position may aggravate this problem. Diabetics are at greater risk.
This nerve can be compressed beneath a ligament, tendon or tight muscle in your hip and pelvis. Pregnancy or being even slightly overweight makes this condition more likely. Tight clothing including girdles, compressive shorts, or tight belts may aggravate or cause this condition. Carpenters’ tool belts or police duty belts may compress this nerve. Prolonged sitting or lying in a fetal position may aggravate this problem. Diabetics are at greater risk.
In the early stages of this condition, your symptoms are usually mild and intermittent. Walking or standing may aggravate the symptoms, and sitting tends to relieve them. In more advanced stages, numbness and tingling changes to shooting pain that is unaffected by your position.
The central goal of treatment is to decrease any cause of compression. In some cases, simply wearing looser clothing or belts may help relieve your symptoms. Some men find relief by switching from a belt to suspenders. Avoid wearing a tool belt or duty belt that places pressure over the area. If you are overweight, begin a sensible weight loss program to avoid compression from excessive tissue.
Chondromalacia Patellae; sounds dramatic, usually isn’t.
The term “Chondromalacia Patellae” (CMP) describes painful damage to the cartilage behind your kneecap. CMP may begin at any age and is commonly found in teenagers. The likelihood of developing CMP increases with age, and the condition is more common in females. You are more likely to develop CMP if you are overweight or have had a prior knee injury.
One of the most common causes of CMP is an imbalance between the muscles that help to guide your kneecap and its “V-shaped” groove at the end of your thigh bone. Repeatedly flexing and extending a misaligned kneecap leads to pain, swelling, and eventually cartilage damage. Misalignment of the kneecap (patella) is often secondary to problems in your hip and foot, especially weakness of your gluteal muscles or flat feet.
CMP causes a dull pain behind your kneecap that is aggravated by prolonged walking, running, squatting, jumping, kneeling, stair climbing, or arising from a seated position. The pain is often worse when walking down hill or down stairs. Popping, grinding, or giving way may occur from long-standing misalignments.
Conservative care, like the type provided in this office, is generally successful at relieving your symptoms. It is important for you to minimize activities that provoke your pain, especially running, jumping, and activities that stress you into a “knock-knee” position. Do not allow your knees to cross in front of your toes when squatting. Some athletes may need to modify their activity to include swimming or bicycling instead of running. Performing your home exercises is one of the most important things that you can do to help recover. The use of home ice or ice massage applied around your kneecap for 10-15 minutes, several times per day, may be helpful.
I’ve got ITB Syndrome Doc! Now What?
Your iliotibial band is a fibrous band of tissue running from the crest of your hip, down to your knee. A muscle near the crest of your hip called the tensor fascia lata, attaches to this band to help control movements of your leg. Your iliotibial band passes over the point of your hip and over another bony bump on the outside of your knee called the lateral epicondyle. When the band is too tight, it can become painfully inflamed as it repeatedly rubs over the top of either of these bony projections. Irritation at the bony bump near the knee is called iliotibial band friction syndrome.

The condition usually presents as pain on the outside of your knee that becomes worse with repetitive knee flexion or extension. This condition is the leading cause of lateral knee pain in runners, especially slower “joggers.” The pain usually develops 10-15 minutes into the workout. You may sometimes feel or hear a click during movement. Symptoms generally ease at rest. Running on slick “wintry” surfaces may aggravate the condition. Excessively worn running shoes may be a culprit.
This problem is commonly caused by weakness in your gluteal muscles. When these muscles are weak, the muscle that attaches to your iliotibial band must contract harder to stabilize your hip. Having one leg longer than another is a known aggravating factor.
Runners should minimize downhill running and avoid running on a banked surface like the crown of a road or indoor track, as well as wet or icy surfaces. Runners should reverse directions on a circular track at least each mile. Bicyclists may need to adjust seat height and avoid “toe in” pedal positions. Avoid using stair climbers or performing squats and dead lifts. Sports cream and home ice massage may provide some relief of symptoms.
Runner’s Knee Sucks.
Patellofemoral pain syndrome (PFPS) describes a painful irritation of the cartilage behind your kneecap. Although anyone may be affected, it is often the result of overuse of the knee in sports that require jumping or running so it is sometimes referred to as “Runner’s knee”. PFPS is the most common cause of knee pain in the general population, affecting an estimated 25% of adults.

One of the most common causes of PFPS is an imbalance between the muscles that help to guide your kneecap in its V-shaped groove at the end of your thigh bone. Repeatedly flexing and extending a misaligned kneecap leads to pain, swelling and eventually arthritis. Misalignment of the kneecap (patella) is often secondary to problems in the hip and foot, especially weakness of your gluteal muscles or flat feet.
PFPS produces a dull pain behind the kneecap that is aggravated by prolonged walking, running, squatting, jumping, stair climbing or arising from a seated position. The pain is often worse when walking downhill or down stairs. Longstanding misalignment can cause damage to the cartilage, which results in popping, grinding or giving way.
Conservative care, like the type provided in this office, is generally successful at relieving your symptoms. Initially, it is important for you to minimize activities that provoke your pain, especially running, jumping and activities that stress you into a “knock-kneed” position. Don’t allow your knees to cross in front of your toes when squatting. Some athletes may need to modify their activity to include swimming or bicycling instead of running.
Performing your home exercises consistently is one of the most important things that you can do to help realign the patella, relieve pain and prevent recurrence. The use of home ice or ice massage applied around your kneecap for 10-15 minutes, several times per day may be helpful.
What is knee tendonitis?
Tendons are strong bands of fibrous tissue that connect your muscles to your bones. Your “patellar tendon” connects your kneecap (patella) to your shin bone (tibia). “Patellar tendonopathy” results from repetitive straining and micro-tearing of this connection, resulting in pain and inflammation. The condition is referred to as “jumper’s knee,” since damage is thought to often result from repetitive jumping.


The condition should probably be called “landing knee,” since forces on the patellar tendon are twice as great during landing as compared to those created during take off.
Patellar tendinopathy is common, affecting almost 20% of all athletes with a rate as high as 50% in sports that require repetitive forceful jumping, like basketball and volleyball. The condition may affect one or both knees and may be slightly more common in males.
Weakness in the quadriceps muscle of your thigh can allow excessive bending of your knee when you land following a jump. This places your patellar tendon at a greater risk for injury. Having strong quadriceps muscles protects your knee from excessive flexion and injury.
Symptoms of patellar tendinopathy include pain or swelling just below your kneecap. This may begin without an identifiable injury and may come and go for months or years. Symptoms are usually aggravated by activity, but most athletes have been able to continue playing through the pain. Pain often increases during activities that require strong quadriceps contraction, like jumping, squatting, arising from a seated position, stair climbing, or running. Walking down stairs or running down hill seems to be more bothersome than going up.
Some athletes may have unconsciously learned to protect their knee by developing unnatural jumping mechanics. This could include landing with a more rigid knee, or allowing too much hip flexion. You may need to become more conscious of landing with the right amount of knee flexion with your foot in a neutral position and avoiding excessive hip flexion. Your doctor would be able to answer any questions you have about good jumping mechanics.
Patellar tendon straps, like a Cho-pat, can help reduce stress on your patellar tendon and relieve pain. Three fourths of the people who use patellar tendon straps for patellar tendinitis report improvement.
Patellar tendinopathy is treatable. Patients who follow a well-planned strengthening program show similar outcomes to those who have undergone surgery for the problem. Initially, you may need to decrease your training intensity to help protect your knee. You should stay away from activities that produce more than mild pain. You should avoid complete rest, as this could actually increase your risk of recurrence. Using ice packs or ice massage for 10-15 minutes at a time, especially following activity, may help to reduce inflammation.
